Hi
I think perhaps I'm even more cynical than you and ask the question of "how many needed it" as I have found what people say they will do VS what they do when the chips are down varies.
I'm even more cynical because all this discussion of the leading edge technologies moving towards painless day in V in V artery delivered surgery being the way to go makes me think:
ok, who suffers and who are the Guinea pigs in the middle. For there are inevitable mistakes and errors associated with learning. For myself (and I just had the choice 2 years ago) I wouldn't touch tissue with a barge pole.
When in 10 years its established sound best practice, when its the gold standard then I'll go for it.
People can (quite rightly) identify that when I had my first valvotomy (in about 1974) it was radical and new surgery. The difference is that
then there was no other choices (except die slowly as the generations before had done).
When something is opaque the only way to attempt to understand it is by inference. My inference is this: in places like the USA where hospitals are profit centers (
shudders) the customers are "given choices", yet to me they are steered towards tissue valve. Yet in places like Norway where the health system is
socialised (meaning free) they have a preference for installing mechanical valve and don't really desire tissue without appropriate mitigating factors.
If you look at the major social and economic indicators the situation for people in Norway is excellent. Ultra low poverty, fantastic levels of social satisfaction and personal happiness, great services and very modern in delivery of all infrastructure.
Then there is the other money trail. I was having a chat over a coffee with my Pathologist mate who mentioned to me that a catheter surgeon said that the traditional thoracic surgeons were loosing patients to catheter surgery. His hospital does Catheter work (
Queensland Public hospitals each specialises in a field within the capital city), while the hospital I went to specalises in thoracic surgery (
I went to the private operated wing of that hospital for my surgery)
The thoracic surgeons are actually losing business to the catheter surgeons because the thoracic surgeons society made a deliberate choice to
not include catheter based surgery in their field of specialisation (in the early days of its emergence). They stuck to the "we do open heart" line. Increasingly surgeries which were done by heart sugeons are being done by catheter. This is now seeming to include valve surgery.
Will Catheter intervention replace OHS? I suspect that the answer is probably yes. Over what time frame is unknown. Will it do so in a timeframe to be of benefit to me - well that answer is no.
Its not even clear that it will be the model of choice. History is littered with the "certanly: this is the future" that never happened.
Lastly, let me put up a bit of inference in my examination of that opaque box that I think makes a case on its own.
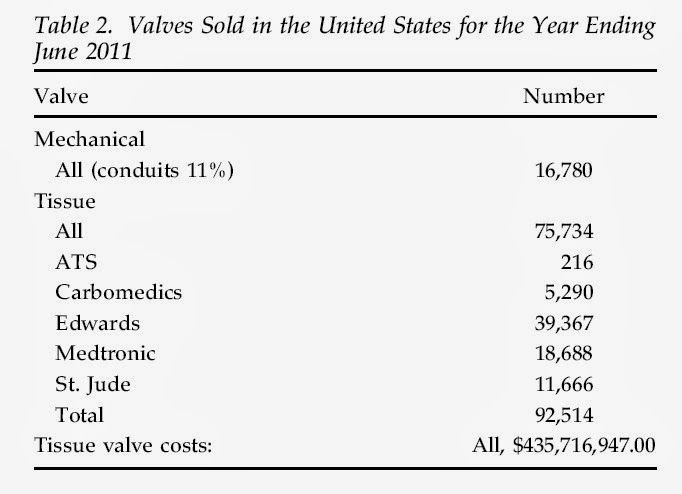
The table column says "Number" yet the bottom number is the addition of all the column and is labeled in $ ... its a little confusing if you ask me. Also, if you do the maths the numbers don't quite add up (507 out) and yet this was published in a "special report" of
Aortic Valve and Ascending Aorta Guidelines for Management and Quality Measures (2013). I guess that wasn't an area where rigor was needed. Still even with a margin of error in the USA tissue valves are big sellers ... each one probably generating repeat business. Its clear to me that for every tissue you fit you'll fit another at least if the patient lives longer. That is largely not true with mechanical.
In this day and age companies who make rugged and long lasting products are far less successful than those who make ones which need to be replaced frequently: its called the throw-away society.
Yet there are people (like me) who choose to buy rugged stuff because when I'm out skiing I don't want my fancy $300 skipole to break OR my
bindings to jam forcing me to walk barefoot (well ok, in thick socks) back across the ice because I can't get my boot off (where we lit a fire to melt them off).
Durability is the key requirement for me in products. I seem to be in the minority and I accept that.
Singer used to make great and rugged sewing machines, we see plastic rubbish now and Singer is extinct. I'm still using Grandmas treddle Singer to repair my tents and backpacks... and I chose a mechanical valve in 2011 for the same reasons.



")