I chose a pig valve when I had mitral valve replacement surgery when I was 44. I was told it would last 10-12 years, then I would need another surgery to replace it again.
The pig valve lasted 18 years- BUT there is a catch: the valve presumably started to fail after 10 years from calcification. My decline was slow and I just thought I was getting old and out of shape.
I insisted my HMO give me an echo-cardiogram every year. The last couple of years they were also giving me ct scans to monitor a node in my lung. So, with all that info that they had collected, my Primary Care provider never told me that the valve was getting more and more calcified, and the cardiologists didn't either. In fact, my last cardiologist told me the valve was starting to leak, and said I would not need another echo for 5 years.
So last May I had an episode where I would run out of breath (badly) just walking a few yards. I was no longer with the HMO (thank God) due to a job change, so I got a top-rated cardiologist in San Francisco to see me through my new PPO. He looked at the latest echo and ct scan, and told me he could see major calcification on the pig valve, and recommended me for surgery to replace it, citing me as an urgent case.
The surgeon he recommended was at Stanford Medical Center, and this guy was amazing. My surgery, which was projected as being 6 hours, took nearly 12. He had to cut through a lot of scar tissue, and my heart was such a mess due to the calcification being so bad, that he had to also do a tricuspid valve repair, and the atrium of my heart was "gigantic", as he said in his post-surgery report. He also told me that I had been sick for a long time with the pig valve failing.
I am lucky to be alive. The surgeon was amazed I lived long enough to make it to surgery, and I almost died on the table. He said I was "a miracle". But my main source of luck was that I was no longer with the HMO (won't tell you which one, but I think they may make aluminum foil as well
")
)
I tell you all this so you know that just accepting the fact that you will need a second surgery down the road with a tissue valve isn't enough. You also need to be aggressively pro-active for yourself with your health care providers, and make sure they are covering all the bases. Other than that, you can pretty much forget that you have a replacement valve in your heart.
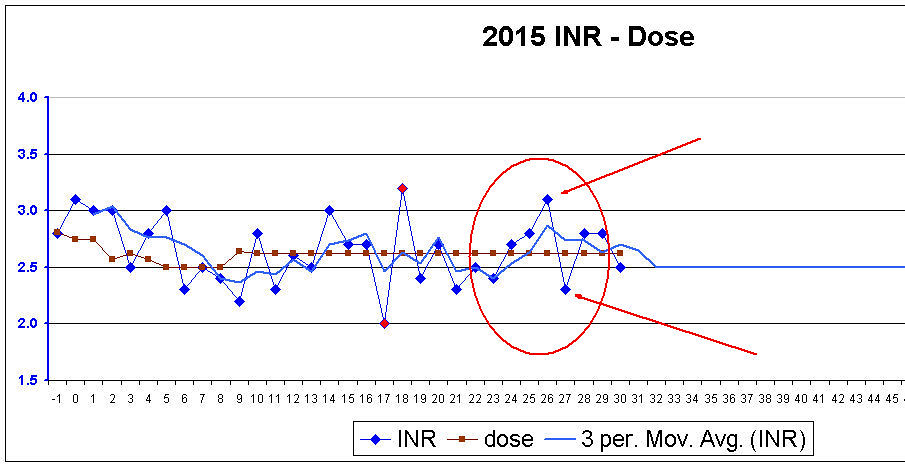
BTW- I chose a mechanical valve this time. I'm now 61, and having to go through this yet again when I am over 70 is just not an option. Obviously, I had to choose the valve prior to surgery, when I didn't really understand just how bad off I was. I just knew how bad I felt. If they had tried to postpone my surgery I would have asked them to just shoot me- I didn't want to keep on living in that condition. So the mechanical valve was the safest option, despite the coumadin issue. I don't regret my choice, even though getting my INR in range had been a pain so far. But my surgery was July 22, so I'm only a month and a half into it.
Hope this helps you make a decision.