| INR | Warfarin (daily mg) |
|---|
average | 2.6 | 7.0516 |
std dev | 0.3 | 0.3 |
max | 3.4 | 7.5 |
min | 1.5 | 6.0 |
over event | 1 | |
under event | 1 | |
inRange % | 96.4 | |
Thanks again for sharing your great results from self monitoring your INR. As you know, I am getting surgery soon and am heavily leaning towards going mechanical. Your data is really helpful as I try to imagine what life will be like on warfarin and gives me confidence that I will be able to self manage and live a normal life.
I was going to start a new thread on this topic, but since this thread has become such a robust discussion about INR management, I thought I would post about some observations, thoughts and questions that I have about the subject.
One thing I am trying to establish is how much my life will be different on warfarin compared to now. Some activities will be off the list, like my boxing. But, also lifestyle. I am not a heavy drinker, but on occasion I do like to have a few. Had 3 glasses of wine with the wife last night. Every now and then that is fun. A few times per month I like to watch the fights at the sports bar(that's pub for some of you) and on those occasions, I will often drink about 6 light beers over the course of 3 hours. I don't like to get drunk, but its enough to keep a buzz and I happen to really like to do that at times. Now, if I listen to some of the doctors giving guidance on drinking alcohol on warfarin, it goes something like this:
"It is best if you don't drink alcohol while on warfarin. But, if you must, never have more than 1 drink. And, whatever you do, do not have more than 2 drinks or you just might die."
Interesting, never once have I found such guidance reference any scientific literature on the subject. And, when I read the numerous threads about the subject on this forum, Pellicle and many others share how they often have a few drinks and guess what?...... they don't die. And beyond that, there seems to be very stable INR readings- certainly in Pellicle's case despite the fact that he likes to throw a few back. Some even report that they go on a bender from time to time, and even they don't report that they have died from it. Ok, I know, participation bias in that only those who survive the bender live to comment on the subject.
")
But, when I search for the evidence, while I did find literature to support that there is an uncommon genetic variant which does cause a person's INR to move significantly from alcohol consumption: Those with VKORC1 1173 C>T, CYP2C9*2 and CYP2C9*3 variant polymorphisms.
For those nerds among us here are some publications on those genotypes:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478047/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4393720/
It seems that this is not present in the vast majority- one study found it to be about 4.2%, linked above. That was among Romanians, which the study indicated was similar to other European populations, but it is found less often in other groups. This seems to make sense, in that most here report no big move in INR from alcohol, but Eva has indicated that hers moves significantly. This is what one would expect from such a distribution.
A conclusion from one of the studies above, which I find interesting given that such a small percentage of this population has this genotype:
" The study also has important implications for improving medication safety. Warfarin had a black box warning about concomitant use of alcohol, but that warning was removed, potentially because of lack of evidence to support the risk of alcohol–warfarin interactions. This study suggests that patients should be warned about alcohol-related warfarin risks. "
Translation: because a very small percentage of the population might get an increase in INR from alcohol, rather than acknowledge that all patients vary and treat our patients like adults, trusting them to establish how alcohol affects their individual INR- give blanket warnings of gloom and doom should you ever dare to drink alcohol.
As I've tried to understand why alcohol makes INR go up for some- the explanation goes something like this based on my reading of the literature- I apologize if this is over simplified: Our liver clears warfarin from our system. When we drink, our liver also now has to contend with clearing alcohol from our system. This causes the liver to be not as effective at clearing warfarin for awhile, especially for some individuals, and can cause warfarin and INR to be elevated for a time. This should not pose a problem for people who drink about the same every day, or whose livers clear medications from their system in a normal way. But, if you have a genetic variant that predisposes your liver to not being able to clear things as well, the alcohol may cause large increases in your INR, especially if you drink erratically.
Here is what I found to be the most comprehensive published paper on the subject attempting to correlate the degree of alcohol consumption to INR above target range. The findings were interesting, but I think not too surprising: In the intro they state: " With regard to warfarin, some, but not all, authors recommend alcohol be avoided completely." Yes, completely.
The study broke the participants into 4 groups depending on their level of alcohol consumption: non-drinkers, light, moderate and heavy. Here is what they found:
" The dose of warfarin required to maintain goal INR levels tended to be slightly higher among men with greater alcohol consumption. " Not surprising. But it also found something that I find even more interesting, but perhaps, not really surprising, unless one subscribes to the guidance that tells you don't drink or you will die: The study found that it did not matter if someone was a non drinker, light drinker, moderate drinker or heavy drinker. There was no correlation between the level of alcohol consumed and the number of INR readings above target, except that heavy drinkers were over INR target less than any of the other groups.
" We found no clear relation between alcohol use and maximal INR levels or the risk of an INR of 2.0 or higher. " (target INR was 1.8 to 2.0)
Results: “ The risks of an INR of 2.0 or higher were 67%, 66%, 68%, and 61% among non-, light, moderate, and heavier drinkers”
Yes, you read that right. The heavy drinkers were over the INR target less than any of the other groups. I am certainly not advocating heavy drinking, but results are results.
Interesting, the researchers could not bring themselves to title their study honestly nor could they bring themselves to say out loud in the conclusion what the results found. Their conclusion was the following: " In summary, among men who had undergone previous CABG surgery, we found little evidence that
moderate alcohol use affects the safety of either lovastatin or lowdose warfarin as measured by ALT and INR levels. " The bold is mine. In truth, they found that no level of alcohol consumption affected the INR, but hey, we sure don't want to even give the appearance of promoting heavy drinking do we, so, let's just leave that part out. There is definitely an anti-alcohol bias in medicine. Like I said, I don't advocate heavy drinking, but don't treat us like children and twist the conclusions of your studies to suit your anti-alcohol bias please.
Here is the study:
https://www.amjmed.com/article/S0002-9343(05)00898-3/pdf
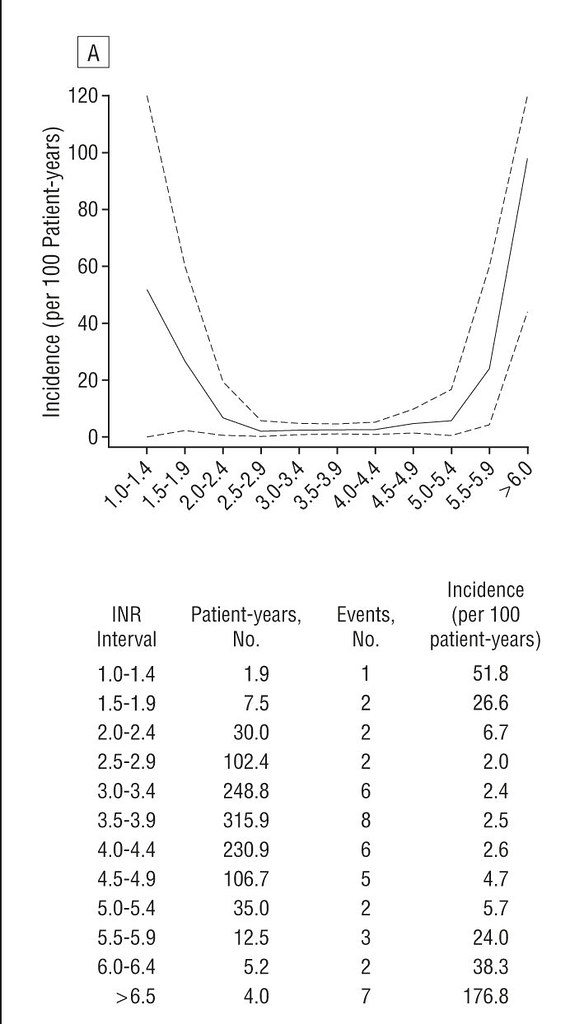
Here is another study which actually found that moderate drinking had a benefit in controlling INR: "Higher vitamin K intake (OR, 0.7; 95% CI, 0.5-0.9) and habitual alcohol consumption of from 1 drink every other day to 2 drinks a day (OR, 0.2; 95% CI, 0.1-0.7) were associated with decreased risk. " for ".... factors independently associated with an INR greater than 6.0"
https://pubmed.ncbi.nlm.nih.gov/9496982/
The data and the feedback here on this wonderful forum seems to suggest, if you drink moderately, you will probably still be able to drink moderately on warfarin. If you like to throw a few back on special occasions, that is probably going to be just fine too.
A question. If a person did find that their INR shot up after having a few drinks in the evening, couldn't adjustments be made to try to stabilize outcomes? For example, let's say mine shoots to 4.0 after drinking a few. With the idea that this is caused by having a little extra circulating warfarin due to delayed processing in the liver, doesn't it make sense that one should be able to plan ahead, through trial and error, and find a way to tweak dose prior to drinking say, drop 1/2 mg for a day or two prior to the big event?
Now, please excuse me. There is an exciting line up for the UFC fights today and I need to make a beer run before they start. I think I'm going to be just fine on warfarin and, if I am one of those genotypes whose INR goes up a lot, I guess I will just have to figure it out.