30% is kind of troubling--especially if the values are HIGH for high INRs and LOW for low INRs. I'm especially concerned about the lower values.
I wonder if the CoaguChek XS has a similar range.
Your question about the CoaguChek XS helped to jog my memory a little. I vaguely remembered an accuracy discussion that came up about the CoaguChek last year, actually before I was even a member here. Now, don't ask how I happen to remember this, I usually forget things my wife tells me within 5 seconds!
Anyway, I would guess it was that thread, and similar posts in a few others, that was subconsciously framing my reference point for what type of accuracy I
assumed these home monitors actually have. I was under the impression that the vast majority (90% or more) of readings were within +/- 10%, so around a 0.3 difference or so. This type of accuracy of course is pretty comfortable, enough to leave a little wiggle room for inaccuracy yet still be in range. So, for reference, I did a quick search and found that thread:
http://www.valvereplacement.org/forums/showthread.php?30821-How-do-you-like-your-Coaguchek-XS.
You'll note two interesting posts in that thread. One mentions that a call to Roche indicated that 30% variance was in fact acceptable. The discussion here recently confirms this - it is actually in the ISO standard. The other interesting post was about Coaguchek XS monitors guaranteeing a maximum difference of 0.3 from lab. So, obviously, some disagreement between the two points.
Well, I just spent a little time researching this further, and so far have not found any mention of the 0.3 guarantee on the official product literature for the CoaguChek XS. I did find a few "expected results" data sets as well as accuracy publications, and they seem to me to indicate much closer to 30% variance than 10%. Anyway, here is what I found:
This CoaguChek page (
http://www.coaguchek.com/com/index.php?target=/en/professionals/further_information/faq/6) mentions possible
deviation as follows: 0.1-0.3 for INR < 2.5 | 0.5-1.0 for INR 2.5 to 4.5 | 1.0 to 2.0 for INR > 4.5. It further says that in general deviations up to +/- 20% are not unusual.
This outside analysis of CoaguChek XS performance (
http://www.coaguchek.com/resource.php?id=Resourcefile-6576494b8e3296faf&f=UkZJTEU2NTc2NDk0YjhlMzI5NjAxNi5wZGY=) that is referenced on the CoaguChek site (
http://www.coaguchek.com/com/index.php?target=/en/professionals/further_information/correlation_studies_and_evaluations) indicates that 97% of values were within the ISO +/- 30% standard. More meaningfully, though, it breaks it down further into the following approximate (there were multiple sets and test strip lots, as well as both blood methods, so I'm just doing a quick eyeball average - see the actual publication for full details) capillary based percentages for INR values less than 4.5: 98% of values were within +/- 30% deviation | 95% of values were within +/- 20% deviation |
67% of values were within +/- 10% deviation.
So, it seems to me that maybe 20% deviation should be considered a reasonably reliable "working range of accuracy". But 10% certainly not. And based on the evidence Roche presents, a 0.3 maximum difference guarantee seems unlikely. I may be wrong, of course, so it would be interesting if any users here could confirm if that's true.
Here's another visual aid on accuracy results, this time for the CoaguChek XS. It's slightly different in format than the INRatio 2 plot earlier, so be careful with direct comparison:



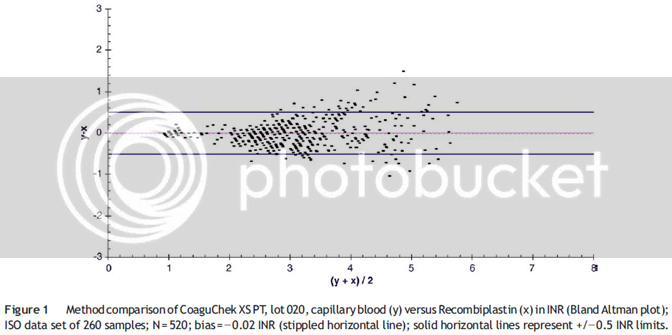
")
