pellicle
Professional Dingbat, Guru and Merkintologist
Having said that, I would like CoaguChek reading to be more aligned with the vein drawn sample going ahead. It has to be consistently reliable so I am not second guessing the results.
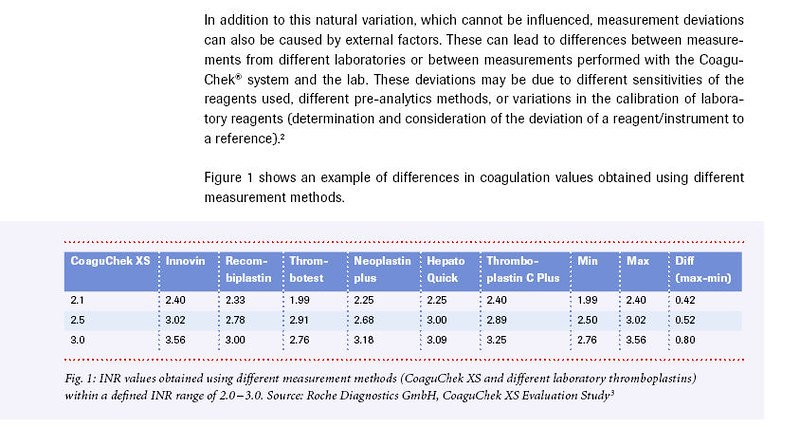
please, do go back up and review that table, it wasn't posted for a teaser.
do you not see the variances in the rows? All of which are vein draws (except the left column which is the Coaguchek?
This is my point, INR is not like measuring a piece of steel with a micrometer. Its by nature rubbery. This is why there is a target and that modern INR management has abandoned the range because people tend to sit on an extreme part of the range if given the chance.
There is always uncertainty and you need to see that "clinically significant" is the point. Move your INR to 2.5 based on the Coaguchek and you'll be in range.
Recall that the Coaguchek also returned 2.3? That's an insignificant difference from a vein draw of 1.9
You didn't mention any possible time difference between the two readings, if it was hours then it could have changed.
Steer towards based on your Coaguchek 2.5 and you'll be fine.
Lastly get another reading with no more than an hour between the two (your Coaguchek and the vein draw time) and see what it is next time? Recently someone els was in a panic about this and it turned out to be the lab.
Last edited: