So I just had a new mechanical valve put in 10 days ago. I was at 2.2 two days ago and get my next test tomorrow morning. I take 7.5mg a day for now. My diet includes a decent amount of Vitamin K via low sodium cold pressed organic vegetable juice that get some a lot of potassium as well as other nutrients every morning and then for lunch I have an Evolution Fresh Cold pressed Green Devotion which also gets me a bunch of potassium, but has spinach and kale with vitamin K. And lastly I eat salads 3-4 days a week for dinner where we use our own home made dressing with avocado oil (know to impact Coumadin). I and trying to figure out how to phase these items back into my diet without sending my INR on a wild ride. I can’t seem to find any guidance on how much vitamin k it takes to impact INR and then how quickly. Thanks for all your suggestions.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
New to Coumadin and vitamin K
- Thread starter Keithl
- Start date



Help Support Valve Replacement Forums:
This site may earn a commission from merchant affiliate
links, including eBay, Amazon, and others.
There is an old, but true, saying among those who have been on warfarin for awhile......."dose the diet and do not try to diet the dose". If you include a lot of vit K in your diet you will probably have to take a higher dose of warfarin to maintain your INR range. Personally, I try to include vit K foods in my diet 5 or so days per week. You will learn, thru trial and erro, how your diet is going to affect your personal INR. Regardless what some say managing INR ain't rocket science. After you have gone 90 days post op look into going to self- testing at home. It is much more convenient and as accurate as lab testing and will get you involved in your personal INR management.
Superman
Well-known member
Echoing Dick’s comments.
Biggest thing to avoiding the roller coaster is consistency. As long as you don’t follow that diet one week, then switch to Keto, then all bread and cheese, you should be able to find a dose that works.
I’ve never heard of a Warfarin dose that’s too high. If 12 mg daily is what it takes, then that’s your dose.
Congrats on the new hardware! May it be the last you’ll ever need.
Biggest thing to avoiding the roller coaster is consistency. As long as you don’t follow that diet one week, then switch to Keto, then all bread and cheese, you should be able to find a dose that works.
I’ve never heard of a Warfarin dose that’s too high. If 12 mg daily is what it takes, then that’s your dose.
Congrats on the new hardware! May it be the last you’ll ever need.
Warrick
Well-known member
I had my valve put in 4th nov 2015 and it was around mid feb 2016 from memory before my INR really settled down, with slight increases from starting 5mg to arrive at around 9 mg daily which is more or less still my dose now with slight alterations week to week, so expect your dose to change.
Ive been taking a vit k supplement for several months now and lately Ive had to drop my dose rather than increase it with vit k.. whod have thunk it...
Ive been taking a vit k supplement for several months now and lately Ive had to drop my dose rather than increase it with vit k.. whod have thunk it...
Last edited:
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
basically (as everyone is suggesting) you simply don't worry about it and eat as you would. The reality is that the minute amounts of vitamin K in foods you eat will make no reproducible difference to your INR.
You can read here:
There are a few things you need to watch though and that's in the main stuff that disturbs the bodys disposal of warfarin (or coumadin if you prefer to say "hoover" than vacuum cleaner), one of these is grapefruit. One member here tweaked to that by drinking a large amount of that.
Thread here : https://www.valvereplacement.org/threads/my-monty-python-moment.42094/
Basically the best approach is to eat what you want (well, lets leave junk food off the list so you're not back with CAB surgery and stick to a good healthy diet) and just test.
The important thing is to test regularly and write it down (I use a spreadsheet, others may prefer a book) so that you can actually reliably keep a track of things and actually reliably pick up any observations (not just coincidences) .
http://www.tylervigen.com/spurious-correlations
Weely testing and a steady hand on dose changes will see you in good stead.
If I haven't already offered my blog post for you to read here it is:
The detailed one which may be a reference:
http://cjeastwd.blogspot.com/2014/09/managing-my-inr.html
and this one which deals with an example:
http://cjeastwd.blogspot.com/2015/10/managing-my-inr-example.html
I have a few others too ...
If you want some help in starting, shoot me a message.
Best Wishes
basically (as everyone is suggesting) you simply don't worry about it and eat as you would. The reality is that the minute amounts of vitamin K in foods you eat will make no reproducible difference to your INR.
You can read here:
- I had a beer and my INR dropped
- I had a beer and my INR rose
- I ate spinach and my INR dropped
- I ate spinach and my INR rose
There are a few things you need to watch though and that's in the main stuff that disturbs the bodys disposal of warfarin (or coumadin if you prefer to say "hoover" than vacuum cleaner), one of these is grapefruit. One member here tweaked to that by drinking a large amount of that.
Thread here : https://www.valvereplacement.org/threads/my-monty-python-moment.42094/
Basically the best approach is to eat what you want (well, lets leave junk food off the list so you're not back with CAB surgery and stick to a good healthy diet) and just test.
The important thing is to test regularly and write it down (I use a spreadsheet, others may prefer a book) so that you can actually reliably keep a track of things and actually reliably pick up any observations (not just coincidences) .
http://www.tylervigen.com/spurious-correlations
Weely testing and a steady hand on dose changes will see you in good stead.
If I haven't already offered my blog post for you to read here it is:
The detailed one which may be a reference:
http://cjeastwd.blogspot.com/2014/09/managing-my-inr.html
and this one which deals with an example:
http://cjeastwd.blogspot.com/2015/10/managing-my-inr-example.html
I have a few others too ...
If you want some help in starting, shoot me a message.
Best Wishes
pellicle
Professional Dingbat, Guru and Merkintologist
Oh and @Keithl
what Warrick says here is correct and common
the change occurs over a few months, which at first worried me as I thought I was building up a tolerance. I asked my Dr and (of course) he was clueless about this stuff (they pretty much all are). It seems the only ones motivated sufficiently to know this stuff are those of us on it (who need to know it).
While posting again I thought you may find this interesting too:
http://cjeastwd.blogspot.com/2017/01/2016-inr-data.html
Best Wishes
what Warrick says here is correct and common
..., with slight increase from starting 5mg to arrive at around 9 mg daily which is more still my dose now with slight alterations week to week, so expect your dose to change.
the change occurs over a few months, which at first worried me as I thought I was building up a tolerance. I asked my Dr and (of course) he was clueless about this stuff (they pretty much all are). It seems the only ones motivated sufficiently to know this stuff are those of us on it (who need to know it).
While posting again I thought you may find this interesting too:
http://cjeastwd.blogspot.com/2017/01/2016-inr-data.html
Best Wishes
Thanks. I had read a lot about consistency and being a stubborn German if there is one thing I am good at, it is consistency. I eat basically sakes things all week long. I need to see where my INR is today and I meet with cardiologist next week, but I already have researched the home testing option and plan on doing combination of lab and home testing to dial this in and then phase back in my usual diet. Being the anal person having had INR tests daily the first 8 days is scary to go a few days no knowing since it has not settled yet.
I also need to follow up with overall labs as I find myself running hot and cold a lot. I wake up hot then am freezing out of the shower and for next hour.
Thank to this forum and everyone's support.
I also need to follow up with overall labs as I find myself running hot and cold a lot. I wake up hot then am freezing out of the shower and for next hour.
Thank to this forum and everyone's support.
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
I've done a whole month on only meat, potatoes and oats ... then done another whole month on greens, salads and meats ... I was unable to identify any consistent INR variations which could be attributed to diet.
Thus, I measure and calculate.
thats a good plan ... I usually test once every 6 months (lately year) against a lab ... my results are clinically insignificantly different.
refer to stoicism freqently (particularly Epictetus) and keep in mind what you can control and what is outside of your ability to control and keep within what you can control.
")
Thanks. I had read a lot about consistency and being a stubborn German if there is one thing I am good at, it is consistency.
I've done a whole month on only meat, potatoes and oats ... then done another whole month on greens, salads and meats ... I was unable to identify any consistent INR variations which could be attributed to diet.
Thus, I measure and calculate.
I need to see where my INR is today and I meet with cardiologist next week, but I already have researched the home testing option and plan on doing combination of lab and home testing to dial this in and then phase back in my usual diet.
thats a good plan ... I usually test once every 6 months (lately year) against a lab ... my results are clinically insignificantly different.
Being the anal person having had INR tests daily the first 8 days is scary to go a few days no knowing since it has not settled yet.
refer to stoicism freqently (particularly Epictetus) and keep in mind what you can control and what is outside of your ability to control and keep within what you can control.
that's a very good plan, as night sweats are something you definitely need to sort out (as not being bad news)I also need to follow up with overall labs as I find myself running hot and cold a lot. I wake up hot then am freezing out of the shower and for next hour.
Congrats on your new valve! I've had my On-X since 2011 and it has been awesome. I like to eat a lot of greens and I found that as long as I am consistent in my diet and supplements, my INR is fine. I will say that right after surgery it took me several months to get the coumadin stabilized, so don't get discouraged if it takes a little while. Get a home INR monitor if you can. I have one and if I feel like my eating has been off, I will check it in addition to my regular schedule.So I just had a new mechanical valve put in 10 days ago. I was at 2.2 two days ago and get my next test tomorrow morning. I take 7.5mg a day for now. My diet includes a decent amount of Vitamin K via low sodium cold pressed organic vegetable juice that get some a lot of potassium as well as other nutrients every morning and then for lunch I have an Evolution Fresh Cold pressed Green Devotion which also gets me a bunch of potassium, but has spinach and kale with vitamin K. And lastly I eat salads 3-4 days a week for dinner where we use our own home made dressing with avocado oil (know to impact Coumadin). I and trying to figure out how to phase these items back into my diet without sending my INR on a wild ride. I can’t seem to find any guidance on how much vitamin k it takes to impact INR and then how quickly. Thanks for all your suggestions.
Your diet seems great. I have a salad every day and love vegetables, so I still eat that way after being on Coumandin since 2005 when I had a mitral valve replacement. As long as you maintain your current diet everything will be fine. In the beginning the INR has to settle down. Mine was all over the place, so don't worry about that. As far as Vit K, if you have some every day that is fine. It is when you stop it for weeks and then decide to go back that is when the INR will be different. Good luck to you and all the best.So I just had a new mechanical valve put in 10 days ago. I was at 2.2 two days ago and get my next test tomorrow morning. I take 7.5mg a day for now. My diet includes a decent amount of Vitamin K via low sodium cold pressed organic vegetable juice that get some a lot of potassium as well as other nutrients every morning and then for lunch I have an Evolution Fresh Cold pressed Green Devotion which also gets me a bunch of potassium, but has spinach and kale with vitamin K. And lastly I eat salads 3-4 days a week for dinner where we use our own home made dressing with avocado oil (know to impact Coumadin). I and trying to figure out how to phase these items back into my diet without sending my INR on a wild ride. I can’t seem to find any guidance on how much vitamin k it takes to impact INR and then how quickly. Thanks for all your suggestions.
Well had a visit to the Coumadin clinic today. First thing that annoyed me was they did a check with a meter the Cougacheck XS Plus. I asked if they draw blood and they said only when over 8 reading. I said you know the meters are not perfectly accurate. She said she did not know anything about that. I will get a blood draw when I go to cardiologist next week. I will chat with cardiologist and probably look for a lab that will draw blood at least periodically.
So seems my body really adopted well as my INR is 3.5 where the Cleveland clinic wants it at 2-3 and I had to argue as they wanted it 2.5 - 3.5. After some review of my r odds they agreed to 2-3. We chatted a bit and I said let's not over react as I want to ramp my diet back up. We discussed what I wanted to add back in and how much Vitamin K that would be so they agreed to cut today from 7.5 to 5 and then back to 7.5 tomorrow as the vitamin K starts to have impact. I get to go back to my healthy diet for quickly and see how the blood checks on Thursday AM.
So seems my body really adopted well as my INR is 3.5 where the Cleveland clinic wants it at 2-3 and I had to argue as they wanted it 2.5 - 3.5. After some review of my r odds they agreed to 2-3. We chatted a bit and I said let's not over react as I want to ramp my diet back up. We discussed what I wanted to add back in and how much Vitamin K that would be so they agreed to cut today from 7.5 to 5 and then back to 7.5 tomorrow as the vitamin K starts to have impact. I get to go back to my healthy diet for quickly and see how the blood checks on Thursday AM.
marvsehn
Active member
These posts are quite helpful. Here is a bit of my experience since 2012. I have a St Jude and try to keep INR 2-3. I take 8.75 to 10 mg warfarin per day, depending on travel / diet. I find that diet is a big deal and brussel sprouts, broccoli ect make quit a difference (for me, each person is different). Consistency is certainly the best policy. I find that a big helping of vitamin k can change INR by .5 (for me) I self test weekly and use a spreadsheet to track and adjust dose (this is a daily calculation and I adjust for a baseline dose (which is weekly). I think the warfarin tablets take 3-4 days to get in and through your body and I adjust my spreadsheet to account for this. Here is my take (for me) on what dose and V-K do to INR, 1 mg of warfarin ups INR about 0.2 over 4 days, one serving of broccoli drops INR about .25 over 1 day. (There is not much info on how this works or the impact) I use a app called Warfarin HTK and MyINR which helps quit a bit. I manage to be 2-3 about 90% and 1.8 to 3.3 100% of the time. I self test weekly using Alere/Abbot.
almost_hectic
Well-known member
I find that diet is a big deal and brussel sprouts, broccoli ect make quit a difference (for me, each person is different). Consistency is certainly the best policy. I find that a big helping of vitamin k can change INR by .5 (for me)
Agreed, I too find it makes a definite difference that I myself have been able to measure, and yes 100% everyone is different, for sure. I would caution anyone against the thinking that vitamin K in your foods makes no difference. To me that sounds like dangerous advice to give someone new to Coumadin.
Too much is made of vit K and warfarin. Dose your diet.....don't DIET your dose.....and use a little common sense. Personally, I like green vegs. and try to eat some most days per week.......but not every day, nor do I measure the amount of foods containing "K".
FYI. I went the first two decades after surgery with no knowledge of the relationship between warfarin and "K"........and lived to talk about it.....
FYI. I went the first two decades after surgery with no knowledge of the relationship between warfarin and "K"........and lived to talk about it.....
pellicle
Professional Dingbat, Guru and Merkintologist
Ok
Lest discuss this...
0.5 INR points is very hard to clearly identify as being causal ... in fact 0.5 INR points is almost clinically insignificant. This is an important term which is why I've bolded it. Such a change is not considered significant in dose changes by a clinic and if you consider it the cause for a dose change then you are micro managing your dose a wee bit much
excellent, and can you explain please how much you adjust and by what amount?
are you sure of this, and how have you established this?
The problem I see with all these discussions is this:
even this chart does not prove that hangings were caused by science research.
Please note that I am not saying you didn't observe this in a proper rigorous manner, I'm just saying that without it you can't be sure of point observations. For instance I observed from my notes in my sheet that it seemed that exersize was related to INR changes. So I bought a Garmin and wore it for 3 years, charting each of my weekly measurements with activity (using 3 possible indicators, steps, active kilo-calories and heart rates) and after 3 years found that there was really no clear trend emerging from my data and certainly nothing which I could reliably say "I compensate by Xmg". Thus I don't say there is anything clearly usable.
So its just easier to adjust my dose based on my weeks findings in line with statistical trends.
While yes we are all different and yes measurement is good it is important to not leap to conclusions where they are not warranted. As well you absolutely need to give readers relative corrections (not absolute) when discussing this or someone is going to read your post and take away "oh, I add 1mg to my dose when I have greens"; when their daily dose is 5 mg or 15mg it will make either a huge or insignificant difference.
Then there is the critically important thing which is why do we take warfarin? Its not to have an INR flat line competition, its to reduce the risks of having a stroke and reduce the damage caused if we have a bleed (note: important point, being on warfarin does not cause bleeds).
We have oodles of data on what this zone of "therapy" is and its more or less like this:
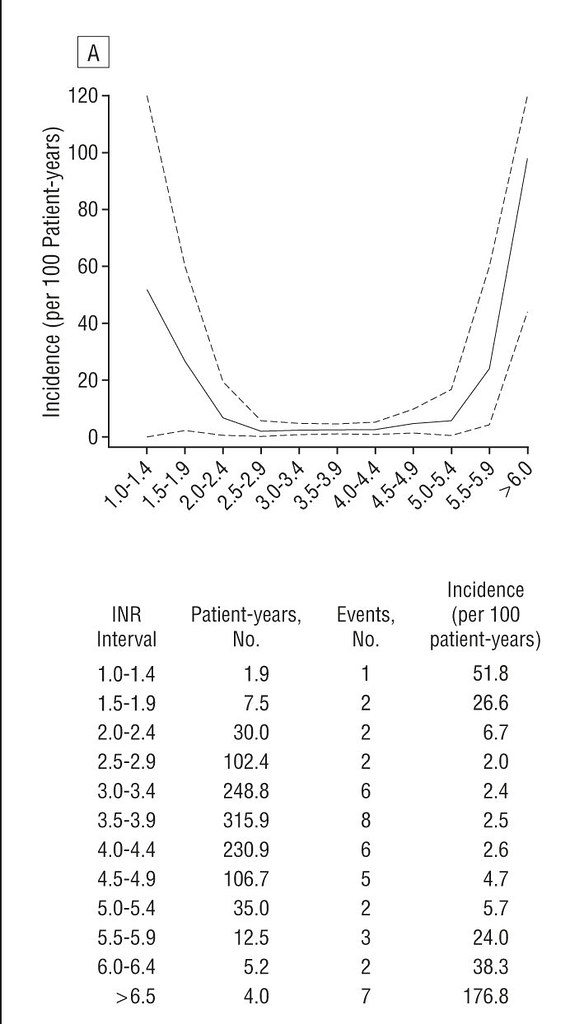
so while your INR may or may not vary much the important point is that as long as your inside this range you've minimised risk sufficiently. Being "more in the middle of the range" is meaningless from a therapeutic basis (remember, we take warfarin for anti-coagulation therapy).
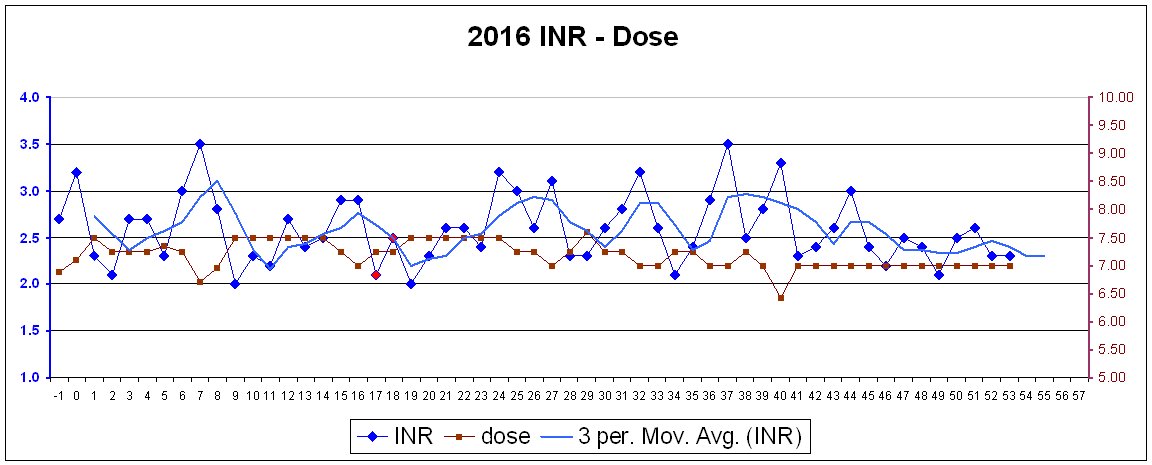
For instance, here is my 2016 data (from daily measurements)
now here is that re-oriented to have the scale of that variance fit within the above curve
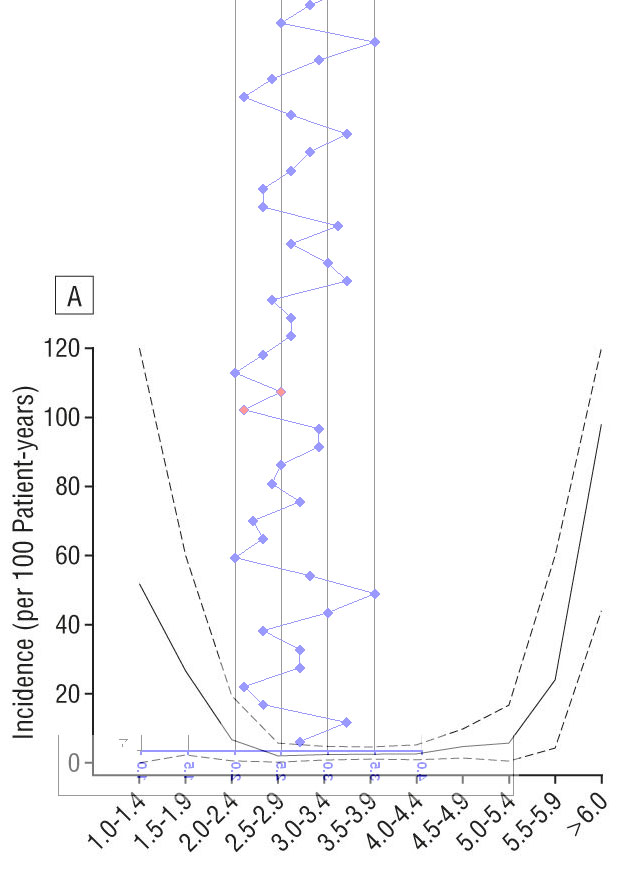
so you can see that while there have been outliers which are close to the edges, I have been inside the statistically safe zone the entire year.
So my view is this: don't over think this or if you are going to (which I encourage) be TOTALLY rigorous and scientific about it. And like science submit your findings and engage in discussion about your findings and accept criticism and iteratively fold that back into your work and your analysis (or its not science, its scientology).
Best Wishes
Lest discuss this...
...I find that a big helping of vitamin k can change INR by .5 (for me)
0.5 INR points is very hard to clearly identify as being causal ... in fact 0.5 INR points is almost clinically insignificant. This is an important term which is why I've bolded it. Such a change is not considered significant in dose changes by a clinic and if you consider it the cause for a dose change then you are micro managing your dose a wee bit much
...I self test weekly and use a spreadsheet to track and adjust dose (this is a daily calculation and I adjust for a baseline dose (which is weekly).
excellent, and can you explain please how much you adjust and by what amount?
I think the warfarin tablets take 3-4 days to get in and through your body and I adjust my spreadsheet to account for this.
are you sure of this, and how have you established this?
1mg up from what base dose please?Here is my take (for me) on what dose and V-K do to INR, 1 mg of warfarin ups INR about 0.2 over 4 days, one serving of broccoli drops INR about .25 over 1 day.
The problem I see with all these discussions is this:
- only the obsessive compulsive or scientifically trained (who were probably a bit OCD on the scale anyway) are likely to do this, most can't even explain how their home dosing strategy is set up to prevent errors let alone actually diligently make measurements
- it engenders in the "hyper-anxious" a feeling that there is so much to do which is incorrect (for one can just eat and take INR and make adjustments when needed ... and its this "when needed" which is the problem and not usually discussed
- most people are bad at correctly identifying a correlation and the first time they think they see one (oh, my INR rose a tiny amount that must have been from the Spinach that I had some days back) they assign causality. The reality is that you need a rigorous approach to actually be sure of that so that you eliminate coincidence.
even this chart does not prove that hangings were caused by science research.
Please note that I am not saying you didn't observe this in a proper rigorous manner, I'm just saying that without it you can't be sure of point observations. For instance I observed from my notes in my sheet that it seemed that exersize was related to INR changes. So I bought a Garmin and wore it for 3 years, charting each of my weekly measurements with activity (using 3 possible indicators, steps, active kilo-calories and heart rates) and after 3 years found that there was really no clear trend emerging from my data and certainly nothing which I could reliably say "I compensate by Xmg". Thus I don't say there is anything clearly usable.
So its just easier to adjust my dose based on my weeks findings in line with statistical trends.
While yes we are all different and yes measurement is good it is important to not leap to conclusions where they are not warranted. As well you absolutely need to give readers relative corrections (not absolute) when discussing this or someone is going to read your post and take away "oh, I add 1mg to my dose when I have greens"; when their daily dose is 5 mg or 15mg it will make either a huge or insignificant difference.
Then there is the critically important thing which is why do we take warfarin? Its not to have an INR flat line competition, its to reduce the risks of having a stroke and reduce the damage caused if we have a bleed (note: important point, being on warfarin does not cause bleeds).
We have oodles of data on what this zone of "therapy" is and its more or less like this:
so while your INR may or may not vary much the important point is that as long as your inside this range you've minimised risk sufficiently. Being "more in the middle of the range" is meaningless from a therapeutic basis (remember, we take warfarin for anti-coagulation therapy).
For instance, here is my 2016 data (from daily measurements)
now here is that re-oriented to have the scale of that variance fit within the above curve
so you can see that while there have been outliers which are close to the edges, I have been inside the statistically safe zone the entire year.
So my view is this: don't over think this or if you are going to (which I encourage) be TOTALLY rigorous and scientific about it. And like science submit your findings and engage in discussion about your findings and accept criticism and iteratively fold that back into your work and your analysis (or its not science, its scientology).
Best Wishes
Last edited:
Superman
Well-known member

pellicle
Professional Dingbat, Guru and Merkintologist
distilled into: eat what you like, test weekly, adjust dose as needed.
coumandin usually makes one cold most of the time.Hi
I've done a whole month on only meat, potatoes and oats ... then done another whole month on greens, salads and meats ... I was unable to identify any consistent INR variations which could be attributed to diet.
Thus, I measure and calculate.
thats a good plan ... I usually test once every 6 months (lately year) against a lab ... my results are clinically insignificantly different.
refer to stoicism freqently (particularly Epictetus) and keep in mind what you can control and what is outside of your ability to control and keep within what you can control.
that's a very good plan, as night sweats are something you definitely need to sort out (as not being bad news)
marvsehn
Active member
Ok
Lest discuss this...
0.5 INR points is very hard to clearly identify as being causal ... in fact 0.5 INR points is almost clinically insignificant. This is an important term which is why I've bolded it. Such a change is not considered significant in dose changes by a clinic and if you consider it the cause for a dose change then you are micro managing your dose a wee bit much
excellent, and can you explain please how much you adjust and by what amount?
are you sure of this, and how have you established this?
1mg up from what base dose please?
The problem I see with all these discussions is this:
For example
- only the obsessive compulsive or scientifically trained (who were probably a bit OCD on the scale anyway) are likely to do this, most can't even explain how their home dosing strategy is set up to prevent errors let alone actually diligently make measurements
- it engenders in the "hyper-anxious" a feeling that there is so much to do which is incorrect (for one can just eat and take INR and make adjustments when needed ... and its this "when needed" which is the problem and not usually discussed
- most people are bad at correctly identifying a correlation and the first time they think they see one (oh, my INR rose a tiny amount that must have been from the Spinach that I had some days back) they assign causality. The reality is that you need a rigorous approach to actually be sure of that so that you eliminate coincidence.
even this chart does not prove that hangings were caused by science research.
Please note that I am not saying you didn't observe this in a proper rigorous manner, I'm just saying that without it you can't be sure of point observations. For instance I observed from my notes in my sheet that it seemed that exersize was related to INR changes. So I bought a Garmin and wore it for 3 years, charting each of my weekly measurements with activity (using 3 possible indicators, steps, active kilo-calories and heart rates) and after 3 years found that there was really no clear trend emerging from my data and certainly nothing which I could reliably say "I compensate by Xmg". Thus I don't say there is anything clearly usable.
So its just easier to adjust my dose based on my weeks findings in line with statistical trends.
While yes we are all different and yes measurement is good it is important to not leap to conclusions where they are not warranted. As well you absolutely need to give readers relative corrections (not absolute) when discussing this or someone is going to read your post and take away "oh, I add 1mg to my dose when I have greens"; when their daily dose is 5 mg or 15mg it will make either a huge or insignificant difference.
Then there is the critically important thing which is why do we take warfarin? Its not to have an INR flat line competition, its to reduce the risks of having a stroke and reduce the damage caused if we have a bleed (note: important point, being on warfarin does not cause bleeds).
We have oodles of data on what this zone of "therapy" is and its more or less like this:
so while your INR may or may not vary much the important point is that as long as your inside this range you've minimised risk sufficiently. Being "more in the middle of the range" is meaningless from a therapeutic basis (remember, we take warfarin for anti-coagulation therapy).
For instance, here is my 2016 data (from daily measurements)
now here is that re-oriented to have the scale of that variance fit within the above curve
so you can see that while there have been outliers which are close to the edges, I have been inside the statistically safe zone the entire year.
So my view is this: don't over think this or if you are going to (which I encourage) be TOTALLY rigorous and scientific about it. And like science submit your findings and engage in discussion about your findings and accept criticism and iteratively fold that back into your work and your analysis (or its not science, its scientology).
Best Wishes
So a good bit of this is personal preference. For me a .5 changes seems significant. When I go from 2.5 to 3 I consider it a move. But not always necessary to change the dose. Depending on what I eat it will impact my INR. Eating 1 spinach salad or 5 during a week will make a difference for me. I like to stay between 2-3 INR and I don't really like 4 or 5. Again my preference. When you cut or fall the higher INR will allow more bleeding issues. Again my preference. Depends how active a person is and what your risk profile might be.
Agian
Well-known member
Science nerd.