My surgeon and cardio both highly recommended a tissue valve for me at age 66. They are all of the opinion that TAVR will be routine by the time I might need a replacement. Sure, there are no guarantees, but they seem convinced of it. I trusted them with my life in the OR, so I don't mind relying on their assurances that if I need a replacement it will be possible via TAVR. My surgeon is 20+ years younger than i am, so he'll be around in all probability should i need a re-do.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Natural or Mechanial
- Thread starter bucks1972
- Start date



Help Support Valve Replacement Forums:
This site may earn a commission from merchant affiliate
links, including eBay, Amazon, and others.
cldlhd
Well-known member
Hey my surgeon is a good bit older than I am.... Beautiful spring day today isn't it Jim
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
I've recently seen some data where a person was taking 100micrograms of K2 daily and from when they began taking it (phased it in from 45micrograms) there was no observable effect on their INR outside the usual variation. The reason that this person was taking it was like theGymGuy's reason => they hoped to stabilise their INR variations.
From Good Old Wikipedia:
note the carbon carbon double bond in the repeating tail of meaquinone (absent in phylloquinone) ... the differences are summarised:
HTH
")
cldlhd;n854448 said:Thanks for the info. Well the multivitamin I take has 200 mcg of both k1 and K2 so that's good . I doubt I need the k1 though as I eat a lot leafy greens.
I've recently seen some data where a person was taking 100micrograms of K2 daily and from when they began taking it (phased it in from 45micrograms) there was no observable effect on their INR outside the usual variation. The reason that this person was taking it was like theGymGuy's reason => they hoped to stabilise their INR variations.
From Good Old Wikipedia:
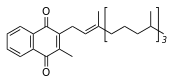
Vitamin K[SUB]1[/SUB] (phylloquinone) - both forms of the vitamin contain a functional naphthoquinone ring and an aliphatic side chain. Phylloquinone has a phytylside chain.
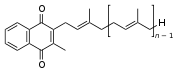
Vitamin K[SUB]2[/SUB] (menaquinone). In menaquinone, the side chain is composed of a varying number of isoprenoidresidues. The most common number of these residues is four, since animal enzymes normally produce menaquinone-4 from plant phylloquinone.
note the carbon carbon double bond in the repeating tail of meaquinone (absent in phylloquinone) ... the differences are summarised:
Vitamin K[SUB]1[/SUB], also known as phylloquinone, phytomenadione, or phytonadione, is synthesized by plants, and is found in highest amounts in green leafy vegetables because it is directly involved in photosynthesis. It may be thought of as the "plant" form of vitamin K. It is active as a vitamin in animals and performs the classic functions of vitamin K, including its activity in the production of blood-clotting proteins. Animals may also convert it to vitamin K[SUB]2[/SUB].
Vitamin K[SUB]2[/SUB], the main storage form in animals, has several subtypes, which differ in isoprenoid chain length. These vitamin K[SUB]2[/SUB] homologues are called menaquinones, and are characterized by the number of isoprenoidresidues in their side chains. Menaquinones are abbreviated MK-n, where M stands for menaquinone, the Kstands for vitamin K, and the n represents the number of isoprenoid side chain residues. For example, menaquinone-4 (abbreviated MK-4) has four isoprene residues in its side chain. Menaquinone-4 (also known as menatetrenone from its four isoprene residues) is the most common type of vitamin K[SUB]2[/SUB] in animal products since MK-4 is normally synthesized from vitamin K[SUB]1[/SUB] in certain animal tissues (arterial walls, pancreas, and testes) by replacement of the phytyl tail with an unsaturated geranylgeranyl tail containing four isopreneunits, thus yielding menaquinone-4. This homolog of vitamin K[SUB]2[/SUB] may have enzyme functions distinct from those of vitamin K[SUB]1[/SUB].
HTH
cldlhd
Well-known member
Then it looks like someone on warfarin would have no adverse effects from taking a K2 supplement, at least up to 100 micrograms ,so that's a good thing.The separate K2 I bought before was mk-7 but the multi doesn't specify.pellicle;n854459 said:Hi
I've recently seen some data where a person was taking 100micrograms of K2 daily and from when they began taking it (phased it in from 45micrograms) there was no observable effect on their INR outside the usual variation. The reason that this person was taking it was like theGymGuy's reason => they hoped to stabilise their INR variations.
From Good Old Wikipedia:
note the carbon carbon double bond in the repeating tail of meaquinone (absent in phylloquinone) ... the differences are summarised:
HTH
pellicle
Professional Dingbat, Guru and Merkintologist
Yeah, it looks that way.cldlhd;n854460 said:Then it looks like someone on warfarin would have no adverse effects from taking a K2 supplement, at least up to 100 micrograms ,so that's a good thing.The separate K2 I bought before was mk-7 but the multi doesn't specify.
The mechanism of action of warfarin is complex (wikipedia has a good summary) but to paraphrase it essentially throws a spanner in the works in a very specific place. Describing this is like explaining internal combustion engines to the point where it is clear to the listener how exhaust extractors work (and drawing upon the physics of trumpet playing).
cldlhd
Well-known member
Well that would be interesting to me (evacuating the spent gases from the cylinder) but I imagine it would be a conversation for another venue.pellicle;n854461 said:Yeah, it looks that way.
The mechanism of action of warfarin is complex (wikipedia has a good summary) but to paraphrase it essentially throws a spanner in the works in a very specific place. Describing this is like explaining internal combustion engines to the point where it is clear to the listener how exhaust extractors work (and drawing upon the physics of trumpet playing).
pellicle
Professional Dingbat, Guru and Merkintologist
Yeah
Hopefully that venue has beer ;-)
But whatI meant was thati you can say to someone "bolt on some extractors to get more power"easily eniough, but explaining why thatwon't "just work" when you then add in a turbo becomes impossible.
Simplifications are good for explaining only something specific. When you expand the parameters you need an entirely new model.
Hopefully that venue has beer ;-)
But whatI meant was thati you can say to someone "bolt on some extractors to get more power"easily eniough, but explaining why thatwon't "just work" when you then add in a turbo becomes impossible.
Simplifications are good for explaining only something specific. When you expand the parameters you need an entirely new model.
MK-7 is the important one to have and 100 mcgs of K2 as MK-7 is the usual dose. If your multi is containing 100 mcgs of K2 as MK-4 then that is an ineffective amount as MK-4 has a half life of only a few hours and people taking K2 as MK-4 need to take several grams of it three times a day. K2 as MK-7 has a half life of several days and only needs taking once a day. I take 200 mcgs per day. Read Dr Kate Rheaume-Bleue's book 'Vitamin K2 and the Calcium Paradox' for lots more information about K2.cldlhd;n854460 said:Then it looks like someone on warfarin would have no adverse effects from taking a K2 supplement, at least up to 100 micrograms ,so that's a good thing.The separate K2 I bought before was mk-7 but the multi doesn't specify.
cldlhd
Well-known member
Thanks I'll check it out. The separate K2 is 90 mcg of mk-7 taken once per day ,the multivitamin is 100 mcg of both k1 and k2 taken twice a day but it doesn't specify any more than that. Maybe I'll shoot them an email and inquire as I'd rather take just the multi .Paleogirl;n854476 said:MK-7 is the important one to have and 100 mcgs of K2 as MK-7 is the usual dose. If your multi is containing 100 mcgs of K2 as MK-4 then that is an ineffective amount as MK-4 has a half life of only a few hours and people taking K2 as MK-4 need to take several grams of it three times a day. K2 as MK-7 has a half life of several days and only needs taking once a day. I take 200 mcgs per day. Read Dr Kate Rheaume-Bleue's book 'Vitamin K2 and the Calcium Paradox' for lots more information about K2.
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
interesting ... I googled that and found the following.
Firstly this study:
http://www.nmcd-journal.com/article/S0939-4753(08)00209-3/abstract
then some other reference which colates a few
http://www.kappabio.com/R-D/CARDIOVASCULAR-DISEASE.aspx
none address the issue of carboxylation of calcium in bone ... which is a common concern for warfarin takers. I have read a recent very technical study on the action of warfarin on VKOR (which happens in the liver) that is responsible for the alteration to coagulation:
I don't disagree the benefits for congestive heart failure that K7 seems to confer, but to me (not seeming to be predisposed to that) the question of bone strength and warfarin is the more compelling one.
Paleogirl;n854476 said:MK-7 is the important one to have and 100 mcgs of K2 as MK-7
interesting ... I googled that and found the following.
Firstly this study:
http://www.nmcd-journal.com/article/S0939-4753(08)00209-3/abstract
then some other reference which colates a few
http://www.kappabio.com/R-D/CARDIOVASCULAR-DISEASE.aspx
none address the issue of carboxylation of calcium in bone ... which is a common concern for warfarin takers. I have read a recent very technical study on the action of warfarin on VKOR (which happens in the liver) that is responsible for the alteration to coagulation:
Within the cell, vitamin K undergoes electron reduction to a reduced form called vitamin K hydroquinone by the enzyme vitamin K epoxide reductase (VKOR)
I don't disagree the benefits for congestive heart failure that K7 seems to confer, but to me (not seeming to be predisposed to that) the question of bone strength and warfarin is the more compelling one.
Hi pellicle how you doing my old sparring partner.
pellicle
Professional Dingbat, Guru and Merkintologist
Good Neil, hope things are good your end too
Agian
Well-known member
What do you mean by 'carboxylation of calcium in bone' and how does this relate to Warfarin?pellicle;n854483 said:none address the issue of carboxylation of calcium in bone ... which is a common concern for warfarin takers. I have read a recent very technical study on the action of warfarin on VKOR (which happens in the liver) that is responsible for the alteration to coagulation:
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
for instance:
Agian;n854526 said:What do you mean by 'carboxylation of calcium in bone' and how does this relate to Warfarin?
for instance:
Title Carboxylated calcium-binding proteins and vitamin K. From a review of recent research involving vitamin K, it is concluded that a new class of proteins has emerged: vitamin K-dependent calcium-binding proteins uniquely characterized by the presence of gamma -carboxyglutamic acid (Gla) residues. Such proteins have been identified in tissues and body fluids and vitamin K-dependent protein carboxylase enzyme activity shares a similarly wide distribution. The highly specialized nature of calcium binding by Gla residues which also promotes protein-phospholipid interaction is important not only in blood coagulation but in many tissue processes involving calcium transport, deposition, homeostasis and calcium-regulated metabolic and physiological activities.
such research stems from interest in correlations between people (in the main, elderly frail sedentary) people on warfarin and those not on warfarin and a higher incidence of osteoporosis.Decreased axial and peripheral bone density in patients taking long-term warfarin
Impaired vitamin K metabolism is associated with under-carboxylation of the non-collagenous bonematrix protein osteocalcin, which is required in its fully carboxylated state for normal bone formation. Post-menopausal women have under-carboxylation of osteocalcin which increases with age and is marked in the elderly. A similarly marked degree of impaired carboxylation occurs during coumarin therapy, and a key question is whether this may lead to accelerated loss of bone mass which is clinically important. We measured axial and peripheral bone mineral density (BMD) in 40 male patients on warfarin and 40 controls individually matched for age, disease and other drug therapy. A consistent trend for reduced BMD at all sites was observed in the warfarin-treated patients. This was particularly marked in the cancellous bone at the distal radius (9% reduction, p=0.023) and at the cancellous rich lumbar spine site (10.4% reduction, p<0.004). No significant relationship was observed between warfarin dose, International Normalized Ratio (INR) or duration of therapy and bone density. Because of the biochemical similarity, this study provides a new lead on post-menopausal osteoporosis, and supports the hypothesis that impaired carboxylation of osteocalcin plays a role in the pathogenesis of bone loss in the elderly through deficiency in vitamin K metabolism
Agian
Well-known member
Thanks Pel. I guess you're thinking there may be other reasons why people on Warfarin may have more fragile bones. For example, they may avoid being active because they don't want to injure themselves.
I believe one of the side effects of warfarin can be (stress, can, not will) osteoporotic fractures. People with osteoporotic fragile bones have to keep active to make their bones stronger, it's very important, but if they're taking a med which might lead to fractures, i.e. warfarin, then that means they have to do more. I believe the reason that warfarin can lead to osteoporotic fractures (I'm not a doctor) is to do with less vitamin K. This is the connection with vitamin K2 and bone health.Agian;n854596 said:I guess you're thinking there may be other reasons why people on Warfarin may have more fragile bones. For example, they may avoid being active because they don't want to injure themselves.
neo
Well-known member
K2 sounds like a good idea, at first. Take a supplement that helps keep calcium away from your tissue, and in the bone. The big question is, does K2 see bovine and porcine tissue the way it sees my tissue? I wouldn't want to assume that K2 would be as helpful for preventing calcification on a bioprosthetic valve as it is for our natural arteries and valves.
bucks1972
Member
Hi this is bucks1972 as a follow-up to me original post. I met with my surgeon yesterday and after some discussion we concluded to go with a tissue valve. His thoughts are by the time I would need a new valve then non-invasive surgery procedures will have been improved to the point as if putting in a stent. So hopefully no open heart. He says I an not a candidate for non-invasive because my age(65) makes me a better candidate for Open heart as my regurgitation of the aortic valve would make it more difficult. He will decide what kind of valve(pig/cow) when during the surgery to ensure the best fit. My surgery is March 25th. once I recovery I will do a post about the journey of anxiety over the last three week from going to what I thought was a healthy person to needing surgery.
March 25th ! That's tomorrow ! If it's then, or whenever, all the very best for a smooth and speedy recovery !