Agian
Well-known member
... and this is why you're so meticulous with your INR, and rightly so.



")
Man, I am getting stressed out.......... I know its not necessarily the case, but I start to feel like I'm a walking time bomb hanging out below range this long.
T
I was out of range today for the first time (1.8) and they seemed very concerned. They doubled my dose today and doubled it tomorrow, so to answer question number one, my sense is they don't want you out of range at all.
Bottom line--it's been a confusing 6 weeks for me.
I have an On-x Aortic valve. I selected that valve specifically to be able to have a more moderated Warfarin dose. My target range is 2-3. I was told as some other that 2.5-3.5 were more typical with other valves. Clinical studies seem to indicate that 2 is the sweet spot to have the lowest combined risk of clot and bleeding. Thus On-X is working to get their valve labeled to recommend 1.5-2.5. Their recently published data seems to support that. Wanting to see more data I like to see my number between 2 and 2.5. Seems like a fair compromise. I did a lot of research on this valve and there are many things about it that make it possible that lower INR targets are a good thing for this valve. In any event, it will be interesting to see how the data develops from the On-X proact trial and future developments.
can you name one? I was under the understanding that the target INR was 2.5 (for that valve and other pyrolytic carbon valves such as the ATS/Medtronics) and that 2 was the lower limit. If you try to sit on 2 you will fail and fall under it.I have an On-x Aortic valve....
Clinical studies seem to indicate that 2 is the sweet spot to have the lowest combined risk of clot and bleeding.
Thus On-X is working to get their valve labeled to recommend 1.5-2.5. Their recently published data seems to support that.
Wanting to see more data I like to see my number between 2 and 2.5. Seems like a fair compromise.
interesting to see how the data develops from the On-X proact trial and future developments.
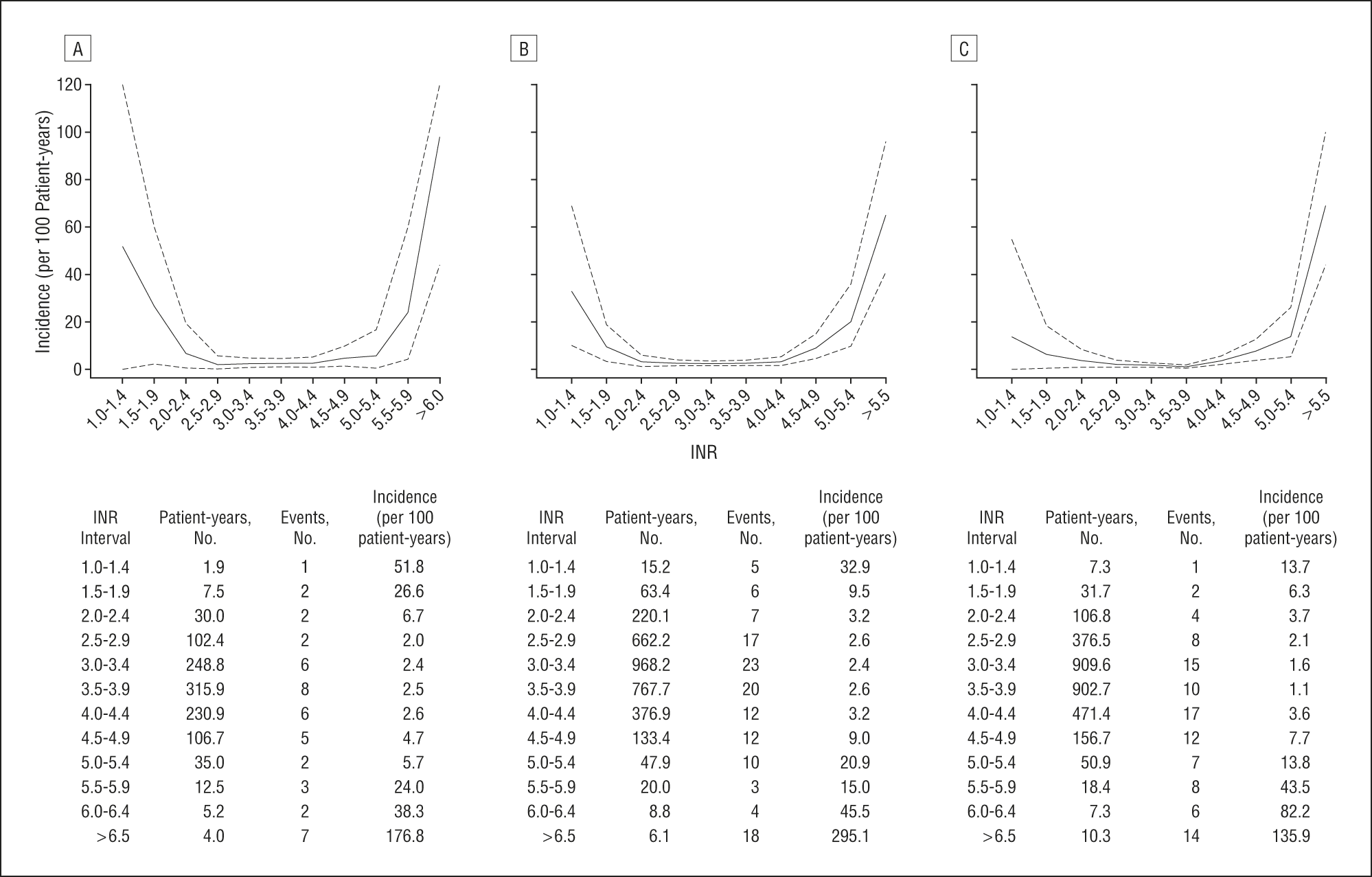
One study I like, particularly for the clear graphs in the figure on page 1207 (page 5 of the actual article) is:
This study included many patients with older valve types, and does not separately summarize results for those with mitral versus aortic valve replacements.
As far as I know, the studies on this are still underway for the aortic valve arm of the ON-X PROACT study. I haven't personally seen any results from the mitral valve arm of the study yet. I believe the arm of the study which was cancelled was only the non-warfarin portion.
Hey, newmitral, a question... the number of mitral valves seems lower than aortic valves, but I can't recally why I think that or if its totally wrong. Perhaps you could set me straight on that one.
The incidence of an event even in the 1.5~1.9 was 26.6 per 100 patient years.
Shudder.
Here is the abstract to the recent publication of the PROACT trial data.
Conclusions
INR can be safely maintained between 1.5 and 2.0 after aortic valve replacement with this approved bileaflet mechanical prosthesis. With low-dose aspirin, this resulted in a significantly lower risk of bleeding, without a significant increase in thromboembolism.
Enter your email address to join: