I am currently dealing with this exact issue with my daughter. For several years she had been taking warfarin manufactured by Taro, and our pharmacy recently switched brands to Teva. My daughter's range for her On-x mitral valve is 2.5-3.5 (though her cardiologist prefers she stay in the 2.5-3.0 range), and she had been staying in that range for months with no problem. Several days after we started the new brand, her INR went to 4.0. I reduced her warfarin by 1 mg that night and rechecked several days later. She had come down to 3.5; I decided to reduce her dosage by another 1 mg that night, and I also REALLY increased her intake of high Vitamin K foods, so imagine my surprise when four days later her INR was up to 4.4. Since there were no other changes in her health, diet, etc., I can only conclude that the different brand warfarin is responsible for the elevated INR. Now I've got to figure out how to recalculate what the new dosage should be going forth with the new brand.true ... but I did want to make the point that its significant to get the right stuff and know that "INR things may change" if the brand changes ...
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
How scared should I be?
- Thread starter Moddeydhoo
- Start date



Help Support Valve Replacement Forums:
This site may earn a commission from merchant affiliate
links, including eBay, Amazon, and others.
true ... but I did want to make the point that its significant to get the right stuff and know that "INR things may change" if the brand changes ...
I disagree. I change brands...no problem. I've had swings in my INR that needed a new permanent dose regimen using pills that came out of the same bottle. INRs can change for reasons nobody knows. Just because B comes after A doesn't mean A caused B.
pellicle
Professional Dingbat, Guru and Merkintologist
Good morning
I guess that you already know this but its just a matter of
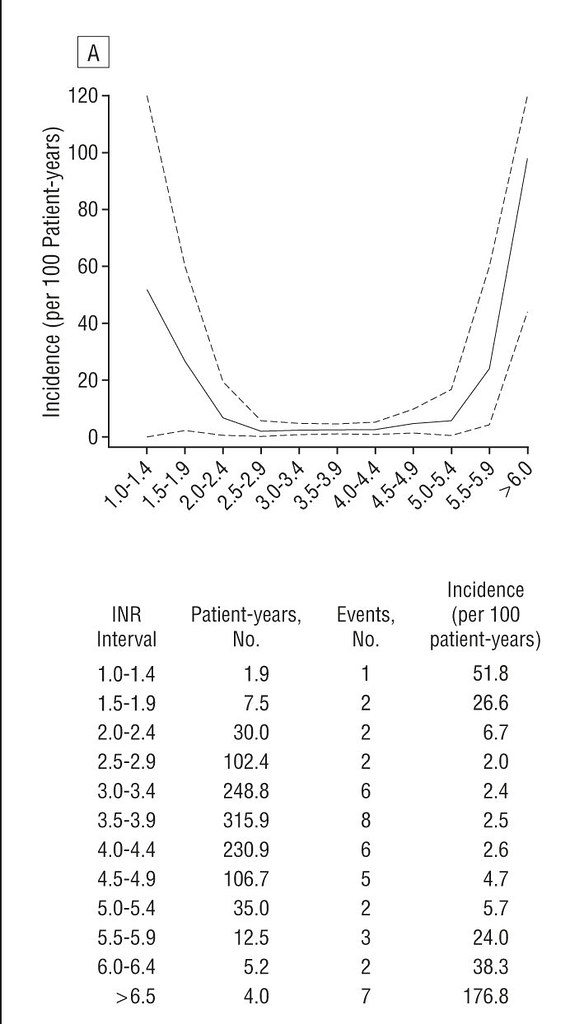
shows that anything up to INR < 4.5 is not statistically more likely for bleeds
Basically the issue is to do with the enantiomers of warfarin. From MIMS on my specific warfarin brand (you'll find similar entries for Warfarin brand too):
then additional information from this source:
so as I say it depends on your brand what you may experience.
Reach out if you have any questions
Best Wishes
... Several days after we started the new brand, her INR went to 4.0. I reduced her warfarin by 1 mg that night and rechecked several days later. She had come down to 3.5; I decided to reduce her dosage by another 1 mg that night, and I also REALLY increased her intake of high Vitamin K foods, so imagine my surprise when four days later her INR was up to 4.4. Since there were no other changes in her health, diet, etc., I can only conclude that the different brand warfarin is responsible for the elevated INR. Now I've got to figure out how to recalculate what the new dosage should be going forth with the new brand.
I guess that you already know this but its just a matter of
- reducing the dose
- waiting a few days before restesting
- deciding if a cycle back to step 1 is needed
shows that anything up to INR < 4.5 is not statistically more likely for bleeds
Basically the issue is to do with the enantiomers of warfarin. From MIMS on my specific warfarin brand (you'll find similar entries for Warfarin brand too):
Marevan is a racemic mixture of the R and S--enantiomers. The S--enantiomer exhibits two to five times more anticoagulant activity than the R--enantiomer in humans, but generally has a more rapid clearance.
then additional information from this source:
During recent years it has been found that one of the possible enantiomers usually has a pharmacological profile that is superior to the racemate. Hence pharmaceutical companies have been replacing exisiting racemic drugs with their pure enantiomeric form.
In the case of Warfarin it was found that S-Warfarin is the superior enantiomer being 6 times more active than R-Warfarin. There are 2 main methods to form a pure enantiomeric form of Warfarin.
so as I say it depends on your brand what you may experience.
Reach out if you have any questions
Best Wishes
Thanks for the info, pellicle. I always call in her results to clinic, so the nurse gave the following advice, with which I concurred:Good morning
I guess that you already know this but its just a matter of
just to perhaps reassure you the INR she's on is not a worringly high INR, for instance
- reducing the dose
- waiting a few days before restesting
- deciding if a cycle back to step 1 is needed
shows that anything up to INR < 4.5 is not statistically more likely for bleeds
Basically the issue is to do with the enantiomers of warfarin. From MIMS on my specific warfarin brand (you'll find similar entries for Warfarin brand too):
Marevan is a racemic mixture of the R and S--enantiomers. The S--enantiomer exhibits two to five times more anticoagulant activity than the R--enantiomer in humans, but generally has a more rapid clearance.
then additional information from this source:
During recent years it has been found that one of the possible enantiomers usually has a pharmacological profile that is superior to the racemate. Hence pharmaceutical companies have been replacing exisiting racemic drugs with their pure enantiomeric form.In the case of Warfarin it was found that S-Warfarin is the superior enantiomer being 6 times more active than R-Warfarin. There are 2 main methods to form a pure enantiomeric form of Warfarin.
so as I say it depends on your brand what you may experience.
Reach out if you have any questions
Best Wishes
The day she tested 4.4, I reduced her wafarin from 6 mg to 1 mg.
I reduced the next night's dose from 6 mg to 5mg.
I will keep tonight's dose at the usual 5 mg.
I will reduce tomorrow night's dose from 6 mg to 5 mg and will re-test the next morning.
Hopefully, this will produce the desired results to get her back in range. What concerns me, though, is how I will be able to calculate what her new daily doses should be moving forward. She had been taking 5 mg on Wednesdays and Saturdays and 6 mg the other five nights of the week. I'm a little perplexed about how best to proceed.
- Joined
- Dec 5, 2020
- Messages
- 2,485
I am sure that Pellicle can guide you through this. He is the INR guru.Thanks for the info, pellicle. I always call in her results to clinic, so the nurse gave the following advice, with which I concurred:
The day she tested 4.4, I reduced her wafarin from 6 mg to 1 mg.
I reduced the next night's dose from 6 mg to 5mg.
I will keep tonight's dose at the usual 5 mg.
I will reduce tomorrow night's dose from 6 mg to 5 mg and will re-test the next morning.
Hopefully, this will produce the desired results to get her back in range. What concerns me, though, is how I will be able to calculate what her new daily doses should be moving forward. She had been taking 5 mg on Wednesdays and Saturdays and 6 mg the other five nights of the week. I'm a little perplexed about how best to proceed.
Just to add my little bit: whilst clearly it is best to be within therapeutic range, personally I would rather be a little over my range than under, as for me the risks seem greater if low. If someone bleeds easily already, or does physically challenging things like trekking or rock climbing, then they may take a different view.
- Joined
- Dec 5, 2020
- Messages
- 2,485
I agree and the graph the Pellicle has shared confirms this. There is a considerable margin of safety on the upside for INR, for most people, and not much margin on the low end before one is in the danger zone.Just to add my little bit: whilst clearly it is best to be within therapeutic range, personally I would rather be a little over my range than under, as for me the risks seem greater if low. If someone bleeds easily already, or does physically challenging things like trekking or rock climbing, then they may take a different view.
I think this ties in with why some are upset with the On-X valve encouraging people to test the lows of INR range. The INR range that they are ostensibly protecting people from is an area with very few actual events. The INR territory that they are expanding into is one with a significant number of events. They better be darn sure of their data before encouraging people to go that low with INR and from what I have seen the data is not convincing.
Last edited:
EMJEF
Active member
- Joined
- Feb 20, 2021
- Messages
- 43
I take 9mg Tues, Thurs, Sat and Sun and then 10mg on Mon, Weds and Fri. My dose has been changed up and down and is always increased/decreased where necessary to bring me in range. At some points I had to take 12mg. I have a 7 day pill box which really helps and have a Coagucheck xs machine.
I’ve always been told that it doesn’t matter on the dose amount, as long as you get to the correct range.
I’ve always been told that it doesn’t matter on the dose amount, as long as you get to the correct range.
pellicle
Professional Dingbat, Guru and Merkintologist
agreedI’ve always been told that it doesn’t matter on the dose amount, as long as you get to the correct range.
I must say however that this alternating dose stuff can (and does) get confusing for people, it takes what should be straight forward and turns it into some sort of Scientology thing (I think I'm going to call this Warfarintology from now on
I take 9mg Tues, Thurs, Sat and Sun and then 10mg on Mon, Weds and Fri
which would be shorter to say
I take 9mg and 10mg alternating
as well you have 9mg (in two consecutive slots which will via some tiny amount) allow a drop meaning why not just take 9.5mg daily and then when you're dishing out your pills you lessen the chances of errors?
EMJEF
Active member
- Joined
- Feb 20, 2021
- Messages
- 43
It works for me and seems to be keeping me in range at the moment.agreed
I must say however that this alternating dose stuff can (and does) get confusing for people, it takes what should be straight forward and turns it into some sort of Scientology thing (I think I'm going to call this Warfarintology from now on
which would be shorter to say
I take 9mg and 10mg alternating
as well you have 9mg (in two consecutive slots which will via some tiny amount) allow a drop meaning why not just take 9.5mg daily and then when you're dishing out your pills you lessen the chances of errors?
- Joined
- Dec 5, 2020
- Messages
- 2,485
It is interesting, because when the Coumadin Clinic lays out my plan for the week, if I am between mg they have me alternate. For much of the past 5 weeks it has been between 3 and 4mg which kept my INR in range and they alternated. I agree with your reasoning to simplify things, and I would just break one 1mg pill in half and set up my idiot box, as someone named it, with 3.5mg for the rest of the week, unless testing showed that I needed something different. For how my own mind works, this simplifies things for me and removes any guesswork as to whether this is a 3mg day or a 4mg day.agreed
I must say however that this alternating dose stuff can (and does) get confusing for people, it takes what should be straight forward and turns it into some sort of Scientology thing (I think I'm going to call this Warfarintology from now on
which would be shorter to say
I take 9mg and 10mg alternating
as well you have 9mg (in two consecutive slots which will via some tiny amount) allow a drop meaning why not just take 9.5mg daily and then when you're dishing out your pills you lessen the chances of errors?
Keeping track of dosing and INR in Excel also helps make sure there is caution to get the dose right, or at least keeping track in a log book.
"Idiot box", hmmmm, I think I like the positive spin term "smart box". I'd truly be lost without my daily pill box, and if that makes me an idiot, so be it.

Last edited:
pellicle
Professional Dingbat, Guru and Merkintologist
Good morning
for sure ... and this sort of alternation is in reality not significant, I have however seen much greater daily differences (more than 30% between days). The adjacent days of the lower dose will make a more significant difference with such profound differences depending on when you test (for instance if testing day was Monday
If you are being told what to do and doing it then it doesn't matter, however if you are actually self managing and are copying an older system put in place it makes the whole thing just 2 more steps confusing for the self manager in training.
We actually do have self managers here, some post here, others here, which inclines me to keep making these sorts of observations.
I'm sorry if I made you feel like it was a personal thing.
It works for me and seems to be keeping me in range at the moment.
for sure ... and this sort of alternation is in reality not significant, I have however seen much greater daily differences (more than 30% between days). The adjacent days of the lower dose will make a more significant difference with such profound differences depending on when you test (for instance if testing day was Monday
If you are being told what to do and doing it then it doesn't matter, however if you are actually self managing and are copying an older system put in place it makes the whole thing just 2 more steps confusing for the self manager in training.
We actually do have self managers here, some post here, others here, which inclines me to keep making these sorts of observations.
I'm sorry if I made you feel like it was a personal thing.
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
On the subject of alternating doses its important to remember that your body does not know about days of the week, so alternations which look good on papermay result in a non alternation on the roll over.
I have seen stuff like this alternating 7 and 3mg. Note that one is a proper alternation and the other is a "humans think in weeks" alternation
nearly 6% difference in daily average
dunno who that was.and set up my idiot box, as someone named it,
On the subject of alternating doses its important to remember that your body does not know about days of the week, so alternations which look good on papermay result in a non alternation on the roll over.
I have seen stuff like this alternating 7 and 3mg. Note that one is a proper alternation and the other is a "humans think in weeks" alternation
Mon | 7 | | Mon | 7 | | |
Tue | 3 | | Tue | 3 | | |
Wed | 7 | | Wed | 7 | | |
Th | 3 | | Th | 3 | | |
Fri | 7 | | Fri | 7 | | |
Sat | 3 | | Sat | 3 | | |
Sun | 7 | | Sun | 7 | | |
Mon | 7 | | Mon | 3 | | |
Tue | 3 | | Tue | 7 | | |
Wed | 7 | | Wed | 3 | | |
Th | 3 | | Th | 7 | | |
Fri | 7 | | Fri | 3 | | |
Sat | 3 | | Sat | 7 | | |
Sun | 7 | | Sun | 3 | | Difference |
daily average | 5.28571428571429 | | daily average | 5 | | -5.71% |
nearly 6% difference in daily average
| | | | | | |
Last edited:
kvinyeta
Member
- Joined
- Apr 12, 2021
- Messages
- 5
I have been on warfarin now for over 2 years now, and am currently on 7.5 mg a day. My dose takes into account my high vitamin K diet (I have a vegetable garden and eat lots of greens out of it every day), as well as a nightly glass of wine with dinner that compensates a bit for the crapton of vegetables I eat. To the original poster I would say to increase the dose until you are at therapeutic range, and will echo Pellicle in saying that this isn't like other drugs where if you increase the dose your body will have some sort of strange adverse reaction. The only thing that can happen is that your blood gets too thin, and that should be monitored until you find the dose that seems reliable for you. The bigger risk is remaining below your therapeutic range. Given that the risk of clots is especially high right after surgery, I am a bit surprised that they were so laissez faire about it. I was not discharged from the hospital until my INR was within range, and had to give myself a heparin shot shortly after being discharged when my INR was below range. My cardiologist has expressly told me it is better to be above range than below, and that is even for me as a very active young person more at risk of cuts/injuries/accidents.
I also wanted to add a couple of things that surprised me and were important lessons for me in regard to INR management, that weren't necessarily discussed by my cardiologist. This is my personal experience, but perhaps may resonate with others here:
1. For me personally, exercise affects my INR. The more I exercise, the faster I metabolize warfarin and my INR goes down. Therefore for me, managing my INR involves a steady(ish) routine of vitamin k intake, exercise and alcohol consumption. If I do more or less of one than usual, then I compensate with the others or adjust my warfarin dose for a day. For example, if I have a lot of greens in a given day and I went for a run, then perhaps the glass of wine is bigger with dinner.
2. The biggest deviations out of range for me with my INR were during periods of very high stress where I didn't eat as much. Not eating as much made my INR go up and out of range. Therefore being congnizant of stress and how it affects your INR may also be important.
I hope you get within range soon and can breathe a sigh of relief!
I also wanted to add a couple of things that surprised me and were important lessons for me in regard to INR management, that weren't necessarily discussed by my cardiologist. This is my personal experience, but perhaps may resonate with others here:
1. For me personally, exercise affects my INR. The more I exercise, the faster I metabolize warfarin and my INR goes down. Therefore for me, managing my INR involves a steady(ish) routine of vitamin k intake, exercise and alcohol consumption. If I do more or less of one than usual, then I compensate with the others or adjust my warfarin dose for a day. For example, if I have a lot of greens in a given day and I went for a run, then perhaps the glass of wine is bigger with dinner.
2. The biggest deviations out of range for me with my INR were during periods of very high stress where I didn't eat as much. Not eating as much made my INR go up and out of range. Therefore being congnizant of stress and how it affects your INR may also be important.
I hope you get within range soon and can breathe a sigh of relief!
- Joined
- Dec 5, 2020
- Messages
- 2,485
Great strategy!if I have a lot of greens in a given day and I went for a run, then perhaps the glass of wine is bigger with dinner.
Attachments

kvinyeta
Member
- Joined
- Apr 12, 2021
- Messages
- 5
Great strategy!
How did you find my picture on the internet?! Hahahahahahah
pellicle
Professional Dingbat, Guru and Merkintologist
Grief tooStress definitely effects INR too. I have noticed when I have been particularly stressed with work or when my nana died my INR changed quite significantly.