It was XS. Roche rep walkEd me through troubleshooting steps. Nothing helped. I was asked to return it. They send me a return package and I returned it though I didn’t have to, since I paid for it!interesting, what was the machine (S or XS), did they ever clarify the actual fault?
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Find one test method and stay with it? Pshaw
- Thread starter Protimenow
- Start date



Help Support Valve Replacement Forums:
This site may earn a commission from merchant affiliate
links, including eBay, Amazon, and others.
pellicle
Professional Dingbat, Guru and Merkintologist
ThanksIt was XS. Roche rep walkEd me through troubleshooting steps. Nothing helped. I was asked to return it. They send me a return package and I returned it though I didn’t have to, since I paid for it!
Interesting
Maybe I'll go back to 6 monthly draws n compares... How old was it?
You’re welcome. Yes, it’s a good idea to compare with lab twice a year.Thanks
Interesting
Maybe I'll go back to 6 monthly draws n compares... How old was it?
I bought mine around end of 2008-March 2020.
Let me reiterate - the two values 'match' if you consider that test results can be considered accurate if they are within +/- 20% of actual values. The value from your meter + 20% and the value of the lab -20% match, with a bit of overlap. The average of the two may be closer to your actual INR.
Even though labs like to give results to two decimal places, there isn't a way to believe, without any doubt, that their results are absolutely correct.
I wouldn't worry about your INR comparing to the lab at this time - either value shows that your actual INR is in range - and that's what you should really focus on.
Repeat the test after a month or so - compare the results at that time. Meters don't usually fail - they're designed to make thousands of tests - and to make each result accurate.
FWIW - I had an issue with my Coag-Sense meters not matching the lab for quite a while. I determined that the lab WAS wrong (for me, and for another patient who was on warfarin), but had other results that were similarly far different from the lab. The results didn't match CoaguChek, either. More recent results were closer to the lab. Did the meter mess up? Was there something in my blood that confused the meter? Who knows.
I had one test where Coag-Sense result was much closer to lab.
I still don't know which is right - Coag-Sense, CoaguChek, or lab - I was told by InRatio - a discontinued, disgraced, meter, to 'trust the labs.' I'm doing this.
But, again, if both labs say that your INR is in range, I'd be comfortable, and not be all that concerned about which method is most accurate.
Even though labs like to give results to two decimal places, there isn't a way to believe, without any doubt, that their results are absolutely correct.
I wouldn't worry about your INR comparing to the lab at this time - either value shows that your actual INR is in range - and that's what you should really focus on.
Repeat the test after a month or so - compare the results at that time. Meters don't usually fail - they're designed to make thousands of tests - and to make each result accurate.
FWIW - I had an issue with my Coag-Sense meters not matching the lab for quite a while. I determined that the lab WAS wrong (for me, and for another patient who was on warfarin), but had other results that were similarly far different from the lab. The results didn't match CoaguChek, either. More recent results were closer to the lab. Did the meter mess up? Was there something in my blood that confused the meter? Who knows.
I had one test where Coag-Sense result was much closer to lab.
I still don't know which is right - Coag-Sense, CoaguChek, or lab - I was told by InRatio - a discontinued, disgraced, meter, to 'trust the labs.' I'm doing this.
But, again, if both labs say that your INR is in range, I'd be comfortable, and not be all that concerned about which method is most accurate.
My HMO has a standing order for a blood draw, so I get my INR tested by the lab every few months.
Because I have CoaguChek XS and Coag-Sense, I usually test weekly, using both meters, and keep track of BOTH results.
Because I have CoaguChek XS and Coag-Sense, I usually test weekly, using both meters, and keep track of BOTH results.
Hi Eva,Thank you Eva! Roche sold to Bio Tel. I could ask Bio Tel I suppose.
I called Roche and they said they use a reagent called Dade Innovin. If Lab corps uses something different that would explain the difference. So how am I supposed to know what Lab corps uses?
Is it all the Lab corps? Or does each have their own?
I know Protime told me not to worry about it. I just thought if I get a low reading on mine at home but its close to the range my doctor won't change anything? I think someone posted something on reagents here on the forum but I don't remember. Was it Pellicle?
Thank you Eva! Roche sold to Bio Tel. I could ask Bio Tel I suppose.
Hi Pellicle,Sheena
I nearly missed this, and would have it this was not a quiet time and I was interested in following @Protimenows posts
if you don't reply to me directly or use an @ mention, then I'll get no notification. Type the @ character then without any space start typing the username, it may take a moment but it will suggest users after 3 letters are typed ...
I have no idea what a Vantus is, but I'll assume that's some amercian company redistributing Roche products and its a Roche Coaguchek
0.7 INR units is a bit more than I'd feel comfortable with but it isn't entirely outside the known possibilities. Firstly, please cast your eyes over this carefully and read the table with care:
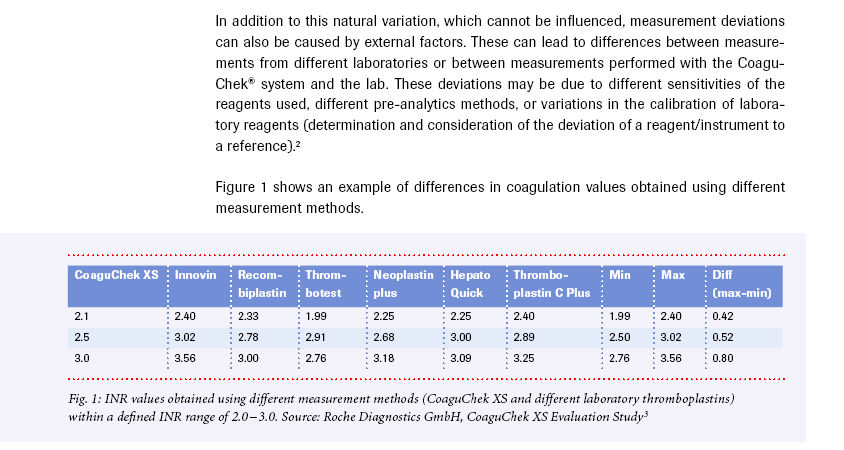
you can see that for a reading of 3.0 on the Coaguchek that the reagent Thrombotest returned 2.76 and Innovin returned 3.56
This is a significant variation within these reagents (reagent is a fancy word for the chemical compound that's used to allow measurement)
You can see that the Coaguchek is between these values.
Now a lab is supposed to do some baseline checks to "tweak" their given result (with their reagent) back up to (probably) WHO guidelines (but I don't know what the USA {or even each state authority} uses). If they have not done the proper "baseline" procedure (because maybe they don't get audited much and who cares right?) then the results you get may be similar to what is in that table (from a Roche publication).
This underscores what I continue to harp about: INR is not a rock, its a bowl of jelly. Do not take measurements of it to be like using a micrometer to measure a piece of steel.
View attachment 887640
I harp about this because I consistently see people (OCD types) fussing about 0.1INR units and trying to skim the edges of their range. It is exactly because of this psychology that the later view of "Target" (not range) was introduced.
Now your Bio does not say if you have a mitral or an aortic (and I can't remember) so what I'd say is to go with your Coaguchek and if you're concerned about it go to a different lab (and ask them the question and a clear and direct way "I had a test somewhere else which gave me a different result to what I expected from another test on the same day, what reagent do you use in your INR testing"
Don't accept any fob offs or walk. That should get them to make sure that they baseline or you can at least compare to that chart.
Back to targets and jelly - I'd always advise staying in the middle of the INR Target as it currently is set by the Surgical Guidelines of your country (which are usually consistent internationally). Aim for the center of the target not the outside ring (which those trying to skim along at the bottom of their range do) and you will naturally account for any possible variances that exist and be in this all important range of outcomes
which according to what you've posted you actually are.
As to what I think you should do, I'd follow your Coaguchek and test again next week and see what that is ... follow up (with an @mention) if you get a result that is perhaps too high and maybe far away from what you want.
Best Wishes
I did a test a week later on my Coagucheck and it was 3.4. I called Roche as Eva suggested and they said it depends on what reagent Labcorps uses? Roche uses Dade Innovin. She said if the lab uses a different reagent that would explain the difference. Honestly how am I supposed to find that out?
And when one travels I thought INR is good internationally. So it depends on reagents?
My difference of .7 last week (2.7 at doc and an hour later at home 3.4) seemed like a lot . Suppose I had a lower read of 2.4 in my machine and my doctor doesn't up my dose, could I then be really much lower? That is my worry. Thank you to you and @ Eva and @Protime for your comments
The reagents will make a difference in results. Although the company provides the reagents, there's no actual target that they use to determine an EXACT value for the reagent. It's more of an educated guess.
Tests by one lab using one reagent and the same lab using a different reagent will often give slightly different results.
The difference in reagent values is the reason why the CoaguChek uses chips to provide an adjustment value.
As far as LabCorp is concerned, all the specimen collection centers do is collect your blood. A courier picks the lab up at the end of day, and transports it to a central lab where the actual testing is done. (I know this because I had a few discussions with them about significant differences between Coag-Sense results and their results - in L. A. County, the blood is transported South of here, near San Diego.)
I've had multiple INRs taken at three or more locations - all with different labs - and the results were usually within .1 - .5 of each other. There IS a variance of values between reagents.
Tests by one lab using one reagent and the same lab using a different reagent will often give slightly different results.
The difference in reagent values is the reason why the CoaguChek uses chips to provide an adjustment value.
As far as LabCorp is concerned, all the specimen collection centers do is collect your blood. A courier picks the lab up at the end of day, and transports it to a central lab where the actual testing is done. (I know this because I had a few discussions with them about significant differences between Coag-Sense results and their results - in L. A. County, the blood is transported South of here, near San Diego.)
I've had multiple INRs taken at three or more locations - all with different labs - and the results were usually within .1 - .5 of each other. There IS a variance of values between reagents.
pellicle
Professional Dingbat, Guru and Merkintologist
you absolutely DO NOT need to ... Did you read that post that you quoted?Honestly how am I supposed to find that out?
And when one travels I thought INR is good internationally
no nothing of the sort ; lets go back to basics here INR means Internation Normalised Ratio: its name is for the professional and scientific community not a consumer name. Once upon a time we used Prothrombin Time (which if you look at your meters manual you will find it does that method too).
It is defined like this:
The INR is derived from prothrombin time (PT) which is calculated as a ratio of the patient’s PT to a control PT standardized for the potency of the thromboplastin reagent developed by the World Health Organization (WHO) using the following formula:
- INR = Patient PT ÷ Control PT
I recommend you also read this: Prothrombin time - Wikipedia
In theory this (if you read that theory) should mean that a reference be applied to it to standardise all reagents, they may not run that process properly, there are (as you saw in my quoted chart) still minor differences.
If you find that confusing then please just ignore all the science accept that 99% of patients are well served by their Roche Coaguchek (and by well served I mean that if they continue to aim for their target and stay in range they are very very unlikely to have any adverse effects from their Anti Coagulation Therapy (ACT).
My difference of .7 last week (2.7 at doc and an hour later at home 3.4) seemed like a lot
while not a "LOT" I'd call it confusing. Both numbers are entirely safe and I strongly suggest you just do your dosing on what your coaguchek reads ... I can give a more complete answer if you wish it
Best Wishes
Last edited:
Sheenas7, at my time it was Roche who called my Lab at UCLA.Hi Eva,
I called Roche and they said they use a reagent called Dade Innovin. If Lab corps uses something different that would explain the difference. So how am I supposed to know what Lab corps uses?
Is it all the Lab corps? Or does each have their own?
I know Protime told me not to worry about it. I just thought if I get a low reading on mine at home but its close to the range my doctor won't change anything? I think someone posted something on reagents here on the forum but I don't remember. Was it Pellicle?
What I started doing since then is to stay above my minimum range and adjust my dose accordingly. My range is 2.5-3.0 (my surgeon said it’s ok to go to 4 in my case). So, I try to keep my INR around 2.9-3.5 using my machine at home.
sometimes this is confusing and troubling, but it will get better with time. Good luck and keep us posted.
Thank you Pellicle. I feel better.you absolutely DO NOT need to ... Did you read that post that you quoted?
no nothing of the sort ; lets go back to basics here INR means Internation Normalised Ratio: its name is for the professional and scientific community not a consumer name. Once upon a time we used Prothrombin Time (which if you look at your meters manual you will find it does that method too).
It is defined like this:
The INR is derived from prothrombin time (PT) which is calculated as a ratio of the patient’s PT to a control PT standardized for the potency of the thromboplastin reagent developed by the World Health Organization (WHO) using the following formula:(*where thromboplastin is the specific word for the more generalised term reagent we throw around here)
- INR = Patient PT ÷ Control PT
I recommend you also read this: Prothrombin time - Wikipedia
In theory this (if you read that theory) should mean that a reference be applied to it to standardise all reagents, they may not run that process properly, there are (as you saw in my quoted chart) still minor differences.
If you find that confusing then please just ignore all the science accept that 99% of patients are well served by their Roche Coaguchek (and by well served I mean that if they continue to aim for their target and stay in range they are very very unlikely to have any adverse effects from their Anti Coagulation Therapy (ACT).
while not a "LOT" I'd call it confusing. Both numbers are entirely safe and I strongly suggest you just do your dosing on what your coaguchek reads ... I can give a more complete answer if you wish it
Best Wishes
- Joined
- Apr 30, 2021
- Messages
- 154
Just started with the coagsense meter and have done several determinations with it. I was getting 2.1 when the Roche machine was reading 2.5. My range is 2 to 3 with first 3 months of valve. I just checked it again yesterday on my coagsense and it was 2.2. Device works real easy with the little pipette tubes. It is kind of fun to do, I’m a sick man.
Amy
Well-known member
- Joined
- Jan 6, 2013
- Messages
- 268
Or maybe there’s a bit of scientist in you.It is kind of fun to do, I’m a sick man.
pellicle
Professional Dingbat, Guru and Merkintologist
I bloody well hope there is :-DOr maybe there’s a bit of scientist in you.
- Joined
- Apr 30, 2021
- Messages
- 154
Bench work can be very tedious. Helps to hone your deductive reasoning with experimental designs. I got a bit of a background as a mad scientist.
Talk about SICK - I had a TIA in 2011 because I trusted a Hemosense meter - it told me 2.6, the hospital said 1.7.
I then went on a quest to find the most accurate meter - I tested CoaguChek S (when they were still available) and XS, Hemosense, ProTime classic and ProTime 3, and, eventually, Coag-Sense Classic. I also compared these blood draws and to the hospital grade machines that my anticoagulation clinic used.
I used a few different labs.
I wanted to find a meter that I trusted my life with.
At that time, my choice was the Coag-Sense, because it seemed to be more accurate at INRs 3 or above than the CoaguChek XS. The results more closely matched the lab results.
I'm still using the Coag-Sense PT2 and the CoaguChek XS; usually within minutes of each other.
In many cases, the CoaguChek XS reports a result that is as much as 1 point higher than the Coag-Sense. Comparing to the labs is hit and miss - sometimes the Coag-Sense is closer to the lab, sometimes it's the XS.
For me, as long as my INR is above 2.5 (on the Coag-Sense) and below about 4.0 (on the XS), I feel comfortable that I'm in a safe range.
I then went on a quest to find the most accurate meter - I tested CoaguChek S (when they were still available) and XS, Hemosense, ProTime classic and ProTime 3, and, eventually, Coag-Sense Classic. I also compared these blood draws and to the hospital grade machines that my anticoagulation clinic used.
I used a few different labs.
I wanted to find a meter that I trusted my life with.
At that time, my choice was the Coag-Sense, because it seemed to be more accurate at INRs 3 or above than the CoaguChek XS. The results more closely matched the lab results.
I'm still using the Coag-Sense PT2 and the CoaguChek XS; usually within minutes of each other.
In many cases, the CoaguChek XS reports a result that is as much as 1 point higher than the Coag-Sense. Comparing to the labs is hit and miss - sometimes the Coag-Sense is closer to the lab, sometimes it's the XS.
For me, as long as my INR is above 2.5 (on the Coag-Sense) and below about 4.0 (on the XS), I feel comfortable that I'm in a safe range.