My initial reason for starting this thread was that therapeutic decisions are based on INR -- and if there was enough difference between INR based on testing, there could be a problem.
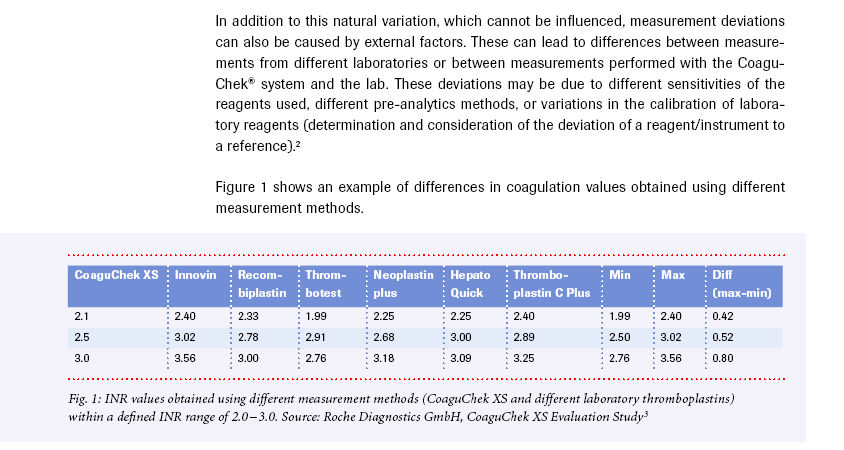
If my Coag-Sense gives me an INR of 3.1, and Coaguchek XS gives a 3.7, and the labs may give an even higher value - trusting the Coag-Sense and making no dosing changes should keep my INR in range. If I responded to the Coaguchek or the labs, I may lower my dosage - without knowing exactly if the reduction in dosage would drop the INR, as tested by the Coag-Sense, would be too high (maybe causing the INR reported by the Coag-Sense to get to 2.0 or lower).
If the difference between the Coag-Sense and the other test methods is a bit troubling -- if all agreed within, say, +/- .2 or .3, this wouldn't be an issue -- but with a difference of 1.0 or higher between Coag-Sense and other methods, dosing differences WOULD be applied, with a potential for moving a person's INR to the top or bottom of a safe range.
In this case, I'm not sure that I overthought this.
If my Coag-Sense gives me an INR of 3.1, and Coaguchek XS gives a 3.7, and the labs may give an even higher value - trusting the Coag-Sense and making no dosing changes should keep my INR in range. If I responded to the Coaguchek or the labs, I may lower my dosage - without knowing exactly if the reduction in dosage would drop the INR, as tested by the Coag-Sense, would be too high (maybe causing the INR reported by the Coag-Sense to get to 2.0 or lower).
If the difference between the Coag-Sense and the other test methods is a bit troubling -- if all agreed within, say, +/- .2 or .3, this wouldn't be an issue -- but with a difference of 1.0 or higher between Coag-Sense and other methods, dosing differences WOULD be applied, with a potential for moving a person's INR to the top or bottom of a safe range.
In this case, I'm not sure that I overthought this.