Thanks. I'd thought that it might be weight based, makes sense.Don't feel bad. My dosing has been all-over the place. I started on 7.5mg in the hospital. Then sent home and was told to take 6mg daily. Holy crud... that let to INR of 4.4. Some weeks my INR is 3.2, or a 2.5. It's all a guessing game till they figure it out.
My doctor has said that Warfarin is weight based... which a lot of it he is right.
Right now I am alternating 2mg 3 days a week and 4mg 4 days a week. I have a feeling it will still be on the high side when I get checked tomorrow.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Dosing Question
- Thread starter Unicusp
- Start date



Help Support Valve Replacement Forums:
This site may earn a commission from merchant affiliate
links, including eBay, Amazon, and others.
Thanks. I may alternate doses like that.5 weeks since surgery may be too soon to expect stability.
Splitting pills is easy, but the active ingredient is not guaranteed to be evenly distributed.
Consistency of dosing and testing is key.
Example :You could try 3 mg 4 days/week (i. e. M/W/F/Su) and 2 mg 3 days per week.
That way you will have the same dose per week and avoid splitting pills.
Test once per week, same test day, same test time each week if possible
Testing more frequently given the lag in INR effect will lead to a desire to "correct" dosing that may be just fine if given enough time to work.
Whatever dose regimen you decide on Don't be too quick to change dose unless way out of safe range.
Also, knowing Pharma, I'd say that the API (Active Pharmaceutical Ingredient) is evenly distributed in the powder blend before they do tablet compression. So not to worry there.
I will try not to be so reactive to dose changes and keep in mind the lag effect. I believe I'm getting closer.
That one beer may be throwing you off! More consistent drinking may help. Just kidding. You could ask for the 1mg tablets. Gives more flexibility in dosing.Exactly... That's what I keep telling the INR nurse but they seem to think that after a month everything should be stable.
I do get tested twice a week (Tuesdays and Fridays). I only have the 2mg pills so no splitting yet. I keep my diet consistent, have one beer a week, but my doctor says they still have me too high on dosing.
Ha!!! Maybe I should be going for the hard liquor instead! Actually on the days I had the beer, my next test my INR was in range at 2.1 and 2.2..... go figure.That one beer may be throwing you off! More consistent drinking may help. Just kidding. You could ask for the 1mg tablets. Gives more flexibility in dosing.
Thanks again Pellicle. Your correct in that we may need to schedule a call. Would be nice to meet.Hi
and please do forgive my little rant about US Dateformat ... bottom line is that if you feel comfortable using it then do so. I happen to use what seems to be US Military format
Dick raises the point on pill boxes, something I also bang on about and am surprised that its not in my own blog post, I believe this post:
https://www.valvereplacement.org/threads/missed-a-dose-what-to-do.865595/post-865636
makes the points well. A search (using Google) will reveal that everyone things its a good idea (except perhaps newbies who think it somehow signals "being old"). Dick makes this point:
https://www.valvereplacement.org/threads/may-have-forgotten-warfarin-for-two-days.887140/post-889115
A pill box is the smartest....and simplest thing we can do to solve one of the biggest problems with warfarin..."did I take my pill today???"....
ok, well I do wish I could talk because talking is much friendlier than typing. So firstly don't make big changes to your dose unless you want big changes to your INR. These changes often take days to sort out.
why are we seeing data for 25th of Feb then?
Anyway its still early days, don't be afraid of the INR being just a weeee tiny bit out of range on the over side and refer again to the graph for why. I would call this an over-reaction
ok, no biggie, I thought it was you who (to my surprise) actually knew their serum albumin ... maybe I got that wrong. Its not really important but as I said in that post its a cornerstone of INR stability and will change as you recover - meaning your dose will change.
well then, as I said there is not sufficient evidence as I saw it to be sure of that. I believe what we are seeing is a yo-yo effect.
I suspect you're saying "what I have on hand is" which isn't quite what I asked. Assuming its what I asked that's a bit gross I'm unaware of any brand that only offers that pair of choices. My brand for instance offers 1 3 & 5. With this selection in your pill colour palate you can make nice sizes easily.
I don't see anything wrong with alternating doses (in your pill box) so that you can do (say) 2.5 | 3 mg if 2.5 is too low and 3 is too high. With such small doses its going to be difficult to shave it in.
I like the new graph
please if you want more than 2 sentence answers and proper answers I encourage you to reach out, >>and we can talk <<
So looking at your new graph I see that you've been adjusting down from an INR of about 4.8 and a dose of 5mg (yes?)
I think I see your logic in dose adjustments there but I disagree with your use of the trendline in such wildly varying data.
INR is creeping up 22 ~ 26th but you've made a rather GROSS adjustment of increasing and or decreasing by 50% ... that's a lot. Tweaking a dose is normally smaller ... like 10% that will be tricky with your dose being so low.
So I would concur with Dick and say alternate 2.5 | 3mg and see what that yeilds. But stay on that for at least 5 days before seeing. Measure as often as you like but if you start moving your dose all over the place it'll be like watching a kid doing a burn out in a rear wheel drive car and slewing all over the place (not a graceful drift like we wish). This is because of the inherent lags in the system.
Lastly, I don't like writing multi page essays only to have my first sentence assumption wrong, second guessing what something means and not really knowing the level of communications best suited to the task.
I don't know why people are afraid to talk and I'm offering to make the call on my coin or WhatsApp which just uses your WiFi.
To make better calls at dosing we need more data (like weeks or months of it) and like I said adjustments should not be made willy nilly because you get the sort of yo yo we're seeing here.
Best Wishes
No issue with the date format. It does make more sense. Just like the metric system that the US claimed was converting to in the early 70's and just never happened. That is more precise too.
Data from 25 Feb: Because that is the day I was released from the hospital and started tracking then. INR was low upon release which is why they had me on 5mg/day. Was just a starting point with no history.
Warfarin dosage here is available in: 1mg/2mg/3mg/4mg/5mg scored tablets assuming that the Pharmacy has them in stock. My Doctor prescribed the first month at 4mg/day in 1mg tablets or 120 tablets. To give me total flexibility in daily dosage. So, I take either 3 - 1mg tabs or 2.5 - 1mg tabs.
Thanks for concurrence on alternating dosage. I'm going to try it for a week and see where I land.
Thanks again. I'll send you a PM when ready to set up a call and we can try to find a good time considering the time difference. Appreciate it.
pellicle
Professional Dingbat, Guru and Merkintologist
Morning
if nothing else it adds a dimension of understanding of tone and style that is absent in ASCII text. I'm told I write in such a way as to sound cranky ... I call it resting bastard text. Some ladies suffer from a related malady
;-)
(I note that the video is considered age restricted .... who the fck is the sensor this lady?

)
dunno, but its sure easier to understand at a glance and do maths with...
normally I'd say more data is helpful, but that original data is really quite meaningless as time goes on and if nothing else it serves to distract.
I keep 1, 3 and 5 because from
Getting back to the issues:
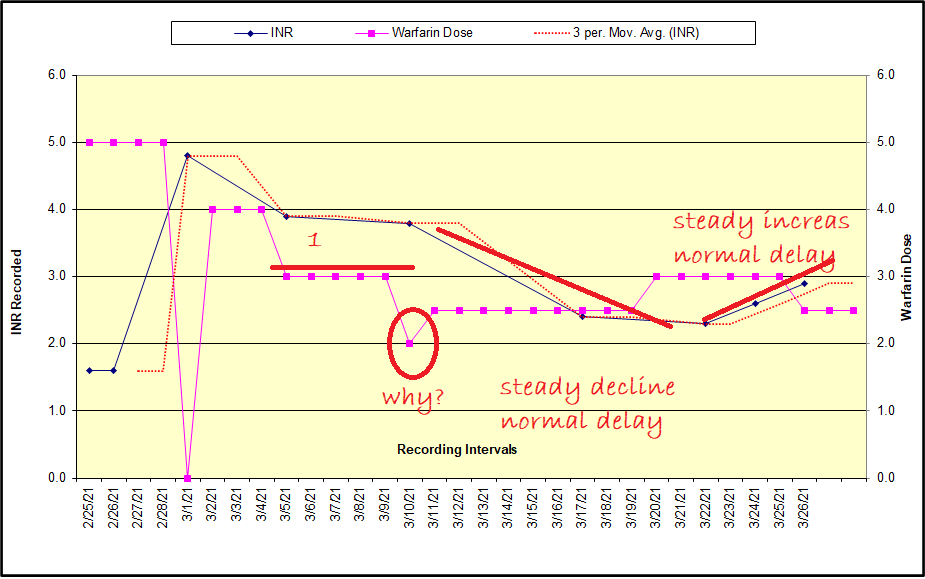
so soon after your surgery I would discount everything left of line marked 1
Next thing to keep in mind (I believe its in my blog posts but perhap buried) is that warfarin has a half life and that half life causes essentially an accumulation over time. Its typically something like this (just based on my dose of 7 for no apparent reason)

so you can see that it takes at least 5 days from taking a dose for the full level of warfarin to "soak in" (balancing ingestion and disposal).
This is then complicated by your changing response to warfarin over the coming months. I was released as stable on 4mg, climbed to 6 for a while, then settled on 7.5 as my median.
Thus (in my blog) I conjecture that (in theory) you'd see an INR like this if all things were equal (which they aren't):

this of course DOES NOT factor in the facts that I just don't know what the lead and lag time for enzyme production in response to altered doses is ... thus the "rule of thumb" (which like all simplifications has limitations) about the dose taking a week to give you a nett effect.
I can't count how many times I've reproduced this above stuff in the many years of my participation across this site ...
I at least get used to saying it ;-)
Would be nice to meet.
if nothing else it adds a dimension of understanding of tone and style that is absent in ASCII text. I'm told I write in such a way as to sound cranky ... I call it resting bastard text. Some ladies suffer from a related malady
;-)
(I note that the video is considered age restricted .... who the fck is the sensor this lady?
)
... Just like the metric system ... That is more precise too.
dunno, but its sure easier to understand at a glance and do maths with...
Data from 25 Feb: Because that is the day I was released from the hospital and started tracking then. INR was low upon release which is why they had me on 5mg/day. Was just a starting point with no history.
normally I'd say more data is helpful, but that original data is really quite meaningless as time goes on and if nothing else it serves to distract.
Warfarin dosage here is available in: 1mg/2mg/3mg/4mg/5mg scored tablets assuming that the Pharmacy has them in stock.
I keep 1, 3 and 5 because from
- 1 > ½
- 3 > 1½
- 5 > 2½
Getting back to the issues:
so soon after your surgery I would discount everything left of line marked 1
Next thing to keep in mind (I believe its in my blog posts but perhap buried) is that warfarin has a half life and that half life causes essentially an accumulation over time. Its typically something like this (just based on my dose of 7 for no apparent reason)
so you can see that it takes at least 5 days from taking a dose for the full level of warfarin to "soak in" (balancing ingestion and disposal).
This is then complicated by your changing response to warfarin over the coming months. I was released as stable on 4mg, climbed to 6 for a while, then settled on 7.5 as my median.
Thus (in my blog) I conjecture that (in theory) you'd see an INR like this if all things were equal (which they aren't):
this of course DOES NOT factor in the facts that I just don't know what the lead and lag time for enzyme production in response to altered doses is ... thus the "rule of thumb" (which like all simplifications has limitations) about the dose taking a week to give you a nett effect.
I can't count how many times I've reproduced this above stuff in the many years of my participation across this site ...
I at least get used to saying it ;-)
As I've said elsewhere, it's not a good practice to alternate doses (I did this years ago before I learned more about Warfarin dosing). The reason is that it causes your INR to fluctuate, depending on the dose you took five days earlier.
This in itself may not be dangerous, but your lab or meter results will vary day by day because the effective dose changes. If you adjust your dosage based on the result (which will fluctuate from day to day because of dosing changes), you might over or under dosage.
There are enough pill dose combinations that it's easy to adjust to a standard daily dose just by splitting pills, if necessary. There's lots of flexibility - go for a daily dose, THEN adjust if you need to.
This in itself may not be dangerous, but your lab or meter results will vary day by day because the effective dose changes. If you adjust your dosage based on the result (which will fluctuate from day to day because of dosing changes), you might over or under dosage.
There are enough pill dose combinations that it's easy to adjust to a standard daily dose just by splitting pills, if necessary. There's lots of flexibility - go for a daily dose, THEN adjust if you need to.
- Joined
- Oct 25, 2020
- Messages
- 66
As a fellow 3 mg/day user, I'll offer/second a couple comments. I was started on warfarin about 20 years ago after throwing some blood clots. The hematologist told me to expect to be on warfarin for life and prescribed me a meter. I subsequently had some AFIB and then 8 years ago received a mechanical valve. For all these years my prescribed dosage has been 3 mg/day. For me personally, I have only found a couple of things that cause appreciable variance.
Firstly, when I was in my 30's I was much more active (competitive distance running). I was probably burning an additional 1K calories per day so I was consuming that much more food (and all that goes with that). That dose was keeping my INR at 1.5-2.0. My point here is that 1000 cal/day difference is quite a bit. Today, eating more or less on any given day, missing a salad, skipping a meal, having more or less beer, etc. does not appreciably change my INR.
Fast forward to today in my late 50's. I've had the valve 8 years and my target INR is 2.5 to 3.5. Honestly, it is very rarely outside of 2.9 to 3.1. Today is my normal test day and it was 3.0. Frankly, for me it is utterly uninteresting . . .. in a good, stable way!
The only things that move my INR today are missing a dose and Tylenol. Yup, I really have missed a dose a handful of times over the years. For me, using that pill box is critical. If I do find I have missed a dose by more than 12 hrs I adjust by 1 mg for 2 days. For someone for whom 3 mg is the stable dose, it is critical to keep in mind that 1 mg is a 33% change.
I believe that most people on warfarin are told to use acetaminophen if needed. There is an interaction but my understanding is for most people it is not a concern. I do not know if it is just my chemistry or if the 3 mg makes me more susceptible but if I take Tylenol for more than a couple of days my INR will move > 0.5. In this case I just adjust from 3 mg to 2 mg. Again, this just my experience.
I'll close with something a consider funny. I lied. My actual prescribed dose is not 3 mg/day. My prescription for the past 8 years has read "take 1 1/2 tablets by mouth once daily except on Friday take 1 tablet". I use 2 mg tablets. After my valve surgery the coumadin clinic decided 20 mg/week was perfect for me. At my annual each year I tell them I just take 3 mg/day but, nope, the prescription never changes.
Firstly, when I was in my 30's I was much more active (competitive distance running). I was probably burning an additional 1K calories per day so I was consuming that much more food (and all that goes with that). That dose was keeping my INR at 1.5-2.0. My point here is that 1000 cal/day difference is quite a bit. Today, eating more or less on any given day, missing a salad, skipping a meal, having more or less beer, etc. does not appreciably change my INR.
Fast forward to today in my late 50's. I've had the valve 8 years and my target INR is 2.5 to 3.5. Honestly, it is very rarely outside of 2.9 to 3.1. Today is my normal test day and it was 3.0. Frankly, for me it is utterly uninteresting . . .. in a good, stable way!
The only things that move my INR today are missing a dose and Tylenol. Yup, I really have missed a dose a handful of times over the years. For me, using that pill box is critical. If I do find I have missed a dose by more than 12 hrs I adjust by 1 mg for 2 days. For someone for whom 3 mg is the stable dose, it is critical to keep in mind that 1 mg is a 33% change.
I believe that most people on warfarin are told to use acetaminophen if needed. There is an interaction but my understanding is for most people it is not a concern. I do not know if it is just my chemistry or if the 3 mg makes me more susceptible but if I take Tylenol for more than a couple of days my INR will move > 0.5. In this case I just adjust from 3 mg to 2 mg. Again, this just my experience.
I'll close with something a consider funny. I lied. My actual prescribed dose is not 3 mg/day. My prescription for the past 8 years has read "take 1 1/2 tablets by mouth once daily except on Friday take 1 tablet". I use 2 mg tablets. After my valve surgery the coumadin clinic decided 20 mg/week was perfect for me. At my annual each year I tell them I just take 3 mg/day but, nope, the prescription never changes.
Thanks. It is more logical so I'm taking your advice. Just cut some 5mg's in half and 1mg's in quarters and will take one of each daily for 2.75mg/day. Will continue for at least 8 days thru next weeks INR test to see impact. Thanks all!As I've said elsewhere, it's not a good practice to alternate doses (I did this years ago before I learned more about Warfarin dosing). The reason is that it causes your INR to fluctuate, depending on the dose you took five days earlier.
This in itself may not be dangerous, but your lab or meter results will vary day by day because the effective dose changes. If you adjust your dosage based on the result (which will fluctuate from day to day because of dosing changes), you might over or under dosage.
There are enough pill dose combinations that it's easy to adjust to a standard daily dose just by splitting pills, if necessary. There's lots of flexibility - go for a daily dose, THEN adjust if you need to.
Thanks for the detailed analysis. And yes, I miss the straight forward total disregard for political correctness in Australia. I prefer blunt straight forward information.if nothing else it adds a dimension of understanding of tone and style that is absent in ASCII text. I'm told I write in such a way as to sound cranky ... I call it resting bastard text. Some ladies suffer from a related malady
Great video. Saw the famous AT&T gal in there. She's made the news lately.
5 weeks since surgery may be too soon to expect stability.
Splitting pills is easy, but the active ingredient is not guaranteed to be evenly distributed.
Consistency of dosing and testing is key.
Example :You could try 3 mg 4 days/week (i. e. M/W/F/Su) and 2 mg 3 days per week.
That way you will have the same dose per week and avoid splitting pills.
Test once per week, same test day, same test time each week if possible
Testing more frequently given the lag in INR effect will lead to a desire to "correct" dosing that may be just fine if given enough time to work.
Whatever dose regimen you decide on Don't be too quick to change dose unless way out of safe range.
Don't know what "guarantee" you want, but the active ingredient in a warfarin tablet is uniformly distributed. Warfarin tablets are made to be split in half; that's why they are scored. They are not made to be split into quarters tho...
I do 4mg T, Th & Sat and 4.5mg M, W, F & Sun. No problem.
the active ingredient in a warfarin tablet is uniformly distributed. Warfarin tablets are made to be split in half
Yeah I know they are made to be split. I first researched this about 10-12 years ago. Many people split tablets and do fine, however my preference based on what I've read is to avoid splitting. Go ahead and split if you don't have the necessary increments in whole tablets, but I would not assume an even distribution in each half.
Some links on the topic:
"Warfarin is NOT evenly distributed within each tablet. As such, doses should be given in whole tablet sizes. Many patients will require alternate day doses e.g. alternating 3mg and 4mg daily, instead of 3.5mg daily." quoted from this: Clinical Haematology : Warfarin Guidelines for Clinicians.
This one is rather ambivalent. Search on 'warfarin" and you'll find the relevant paragraphs
https://www.jmcp.org/doi/pdf/10.18553/jmcp.2009.15.3.272
This one is specific to child dosing, but lands on the side of not splitting if possible. Rather detailed read. Just go to the end and read conclusions. https://www.mdpi.com/1999-4923/12/4/375/pdf
It's been a topic on this forum before. There will always be disagreement on this.
Yeah I know they are made to be split. I first researched this about 10-12 years ago. Many people split tablets and do fine, however my preference based on what I've read is to avoid splitting. Go ahead and split if you don't have the necessary increments in whole tablets, but I would not assume an even distribution in each half.
Some links on the topic:
"Warfarin is NOT evenly distributed within each tablet. As such, doses should be given in whole tablet sizes. Many patients will require alternate day doses e.g. alternating 3mg and 4mg daily, instead of 3.5mg daily." quoted from this: Clinical Haematology : Warfarin Guidelines for Clinicians.
This one is rather ambivalent. Search on 'warfarin" and you'll find the relevant paragraphs
https://www.jmcp.org/doi/pdf/10.18553/jmcp.2009.15.3.272
This one is specific to child dosing, but lands on the side of not splitting if possible. Rather detailed read. Just go to the end and read conclusions. https://www.mdpi.com/1999-4923/12/4/375/pdf
It's been a topic on this forum before. There will always be disagreement on this.
The quote offers no proof or reference for their statement. It does not come from someone schooled in the manufacture of pharmaceuticals or warfarin but from a Clinical Haematology Department.
One paper is titled "Tablet Splitting: Much Ado About Nothing?" For warfarin the answer is yes.
What they all ignore is that when it comes to routine warfarin dosing, when the patient splits a dose they use the other half the next day. So even if the patient splits the pill inaccurately or if warfarin is unevenly distributed (it's not), you'll get the little bit less or little bit extra the next day. Blood concentrations of low dose warfarin in patients are not subject to drastic changes in short periods of time due to human metabolism. So a little bit more on Tuesday and a little bit less on Wednesday has no effect. However, the tablet is meant to be split in half not thirds
pellicle
Professional Dingbat, Guru and Merkintologist
What they all ignore is that when it comes to routine warfarin dosing, when the patient splits a dose they use the other half the next day. So even if the patient splits the pill inaccurately or if warfarin is unevenly distributed (it's not), you'll get the little bit less or little bit extra the next day
THIS!!
- Joined
- Oct 25, 2020
- Messages
- 66
Agree completely. I have never used anything but 2 mg tablets for a 3 mg daily dose so I have a split 100% of the time over many years. Never considered the ingredient distribution within the pill. However, I just split by hand and it is not unusual to be able to visually see that my two halves are not identical in size. Never once worried about it because it just goes in the next pill box space.
................ Never once worried about it because it just goes in the next pill box space.
Exactly!
