I have had a home inr testing machine for the last 8 years of the 25 that I have been on Warfarin and recently became concerned about discrepancies in inr from the lab versus coaguchek xs. I was never told to occasionally verify my home machine with a lab test and never thought otherwise because even when I rarely got checked at my cardio, they also used a coaguchek xs, so I just assumed the machine was accurate. After reading this forum and having labs done at the dr which differed from my machine, I decided to get labs and use my machine within 30 minutes of each other to see the results. I was only able to do this 4 times before my new cardio told me to stop using the machine because my home machine was significantly higher than the lab results. My first test was a 2.5 on the coaguchek and a 2.0 from the lab. The next test was 3.3 on the machine and a 2.5 from the lab. The third test was a 3.6 on the machine and a 2.75 from the lab. The final test was a 3.8 on the machine and a 3.0 from the lab. Each of these tests varies by approximately 20% from the lab values, which I have heard is exceptable but to me this is a problem at any coaguchek measurment that is below 2.5. This potentially means that my real inr is below 2.0 which is not a good thing. This is something that has potentially been going on for nearly 8 years and could have caused serious problems. Luckily for me my old cardio had me between 2.5 and 3.5 which meant even though I was measuring on the Coaguchek, more than likely my real value was above 2.0 as long as my machines reading was 2.5. I have come too find out from a few other cardio's that I should be at an inr bewteen 2.0 and 3.0, so using my machine to regulate my inr at this new range could be a serious problem at anything below 2.5. I am not against using home inr but I would definitely suggest occasionally verify your home results with those of a labs. I also want to say that I used the strips provided by my inr testing company and used strips from different batches. I told the home monitoring company about this issue and they said they are gonna give me another machine but that was weeks ago. I love home monitoring and hopefully I will have different results with a new machine.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Discrepancies in INR between Coaguchek XS and Lab
- Thread starter Cmf2p
- Start date



Help Support Valve Replacement Forums:
This site may earn a commission from merchant affiliate
links, including eBay, Amazon, and others.
pellicle
Professional Dingbat, Guru and Merkintologist
just a point first: lengthy slabs of unformatted text are bloody hard to read.
the use of a new line to break such a thing up helps the reader (who is not just a set of text on a screen, but a real person giving up their time to help you at your request).
Firstly how much experience do you have with the machine? I found that when I first started my reproduction was a bit haphazard. Remember you are being a technician here, not just changing channels with a remote control. You need to make sure that:
Next, I will say that it is well established that labs may not correspond to readings from the XS, this does not mean the XS is not accurate, it may mean that the Lab is not accurate (for it may not have strictly fully followed the proper procedures. Roche has this to say on the topic:

and in earlier publications
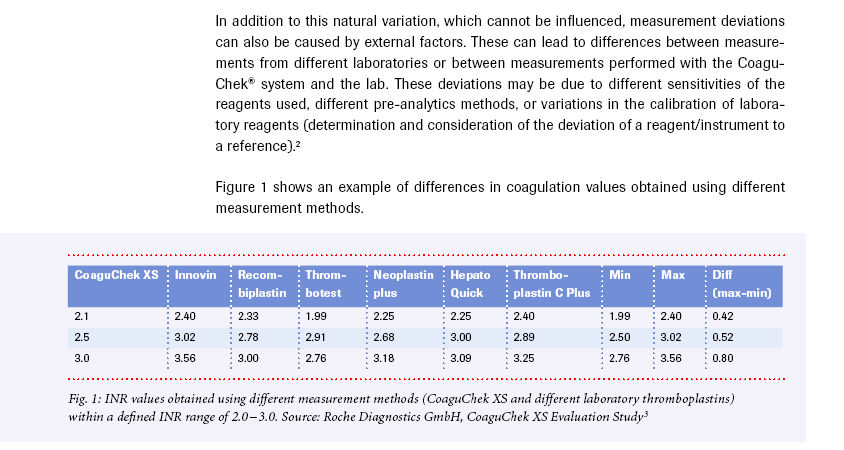
read that carefully word by word and then read the table.
Next we know that the important thing is your INR be kept close to target, modern practice on this is to eschew ranges which is because:

Lastly keep in mind that all that matters is what is significant for "clinical results" (NB you don't have any strokes or thrombosis issues), and so what your INR "actually is" is is of less significance than trends.
See how you go and give me a yell if you're still having trouble.
I hope this helps
the use of a new line to break such a thing up helps the reader (who is not just a set of text on a screen, but a real person giving up their time to help you at your request).
Firstly how much experience do you have with the machine? I found that when I first started my reproduction was a bit haphazard. Remember you are being a technician here, not just changing channels with a remote control. You need to make sure that:
- you are strictly following the directions, including (perhaps especially) the 15 second rule
- you are not milking the finger excessively (which can trigger thrombosis to have started already)
- you are not using the same lance site for subsequent readings (because this will pollute the readings)
Next, I will say that it is well established that labs may not correspond to readings from the XS, this does not mean the XS is not accurate, it may mean that the Lab is not accurate (for it may not have strictly fully followed the proper procedures. Roche has this to say on the topic:
and in earlier publications
read that carefully word by word and then read the table.
Next we know that the important thing is your INR be kept close to target, modern practice on this is to eschew ranges which is because:
- people sit on the boundaries of the range thinking that's good
- the measured INR is not like measuring steel, the more you explore what INR even means the more you'll know this
- the known variance of INR becomes more fuzzy as you get away from INR=2
Lastly keep in mind that all that matters is what is significant for "clinical results" (NB you don't have any strokes or thrombosis issues), and so what your INR "actually is" is is of less significance than trends.
See how you go and give me a yell if you're still having trouble.
I hope this helps
just a point first: lengthy slabs of unformatted text are bloody hard to read.
the use of a new line to break such a thing up helps the reader (who is not just a set of text on a screen, but a real person giving up their time to help you at your request).
Firstly how much experience do you have with the machine? I found that when I first started my reproduction was a bit haphazard. Remember you are being a technician here, not just changing channels with a remote control. You need to make sure that:
- you are strictly following the directions, including (perhaps especially) the 15 second rule
- you are not milking the finger excessively (which can trigger thrombosis to have started already)
- you are not using the same lance site for subsequent readings (because this will pollute the readings)
Next, I will say that it is well established that labs may not correspond to readings from the XS, this does not mean the XS is not accurate, it may mean that the Lab is not accurate (for it may not have strictly fully followed the proper procedures. Roche has this to say on the topic:
View attachment 888292
and in earlier publications
read that carefully word by word and then read the table.
Next we know that the important thing is your INR be kept close to target, modern practice on this is to eschew ranges which is because:
take this graph and trace any point to LHS axis and RHS axis to see what I mean
- people sit on the boundaries of the range thinking that's good
- the measured INR is not like measuring steel, the more you explore what INR even means the more you'll know this
- the known variance of INR becomes more fuzzy as you get away from INR=2
View attachment 888294
Lastly keep in mind that all that matters is what is significant for "clinical results" (NB you don't have any strokes or thrombosis issues), and so what your INR "actually is" is is of less significance than trends.
See how you go and give me a yell if you're still having trouble.
I hope this helps
I appreciate your insight into the matter and I have been doing this for over 8 years on a weekly basis. I understand the instructions for using the machine and do my best to follow the proper procedure.
Looking back on various lab tests over the last year, done at different hospital labs, there is a common trend toward the coaguchek always being significantly higher than the reported lab values when it comes to my blood. I am not saying this is always the case for everyone, just that anyone who is home testing would benefit from occasionally verifying the accuracy of their results by using other proven testing methods.
In my case, my coaguchek xs always reads significantly higher than a lab test, which has never been a problem because my inr has always been around 3.0 to 3.5 on my coaguchek, which was fine because the lab value would be anywhere from 2.3 to 2.8, though this was not known at the time. It has now become a problem because my new cardio wants me at a range of 2.0 to 3.0, instead of 2.5 to 3.5, which is what my old cardio had me at.
I do not feel comfortable trusting my machine if it tells me my inr is 2.0 to 2.5 because this could possibly mean that my true inr is below 2.0, which we all know leads to possible complications over a longer period of time at levels below 2.0. I have a lot more faith in hospital labs that run inr tests all day everyday, than I do in a machine that I use once a week.
In my case it would be potentially dangerous to have my inr trending between 2.0 and 2.5 on my coaguchek, even though these results would be within the acceptable inr range for my condition. I am hoping that my machine is broken or just old and that a new machine will correlate more closely to lab results.
Looking at the graph you posted, my numbers would be extreme outliers when compared to the plotted inr numbers in the graph. This is un settling to me and makes it very difficult to trust that any readings under 2.5 on the coaguchek have me in a safe inr range.
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
I was not to know that and if you'd started with something like that I may have answered differently
pardon the out of order but:
I often recommend this here and do it myself. In my case I'm not more than 0.2 INR units out (although I was 0.5 when I first started.
I'm not sure what you mean by various lab tests, it could mean "various tests at the same lab" or "various labs"
I can only suggest that you can't know without taking readings within hours and documenting them so that you know it was 0.x different
There have been a few people here before who are unable to get consistent lab results but some of those have proven to vanish when they change labs.
I'm a bit confused here:
so are you saying that when you are reading 3.0 on the XS you are seeing 2.3 at the lab? are you sure of these correlations (like you wrote them down with dates?
well I'm not entirely sure I see the problem especially when you don't know what a 2.0 on the XS actually correlates to from a lab (or if you do you haven't said that. Recall from the graphs above that the lower the INR the less the deviation?
agreed, so if you see a trend downwards from 2.5 towards 2 then steer it back up ... if you test weekly there will be no longer period of time
citing a section of "that graph"

would suggest that 6.7 events per 100 patient years is a low risk especially if you steer it up
up to you ... its not been my experience.
I would doubt it, but it could be eliminated by finding somehwere / someone with an XS and taking your strips and code chip there and actually testing side by side.
not so extreme as to not appear on that graph

assuming you know that INR is not like measuring a peice of machined steel with a vernier caliper I suggest its not as unsettling as you feel it is.
I would suggest you follow up and also try (if you already haven't) other labs and see (if you can do so) how much variance you find between companies with a blood draw the same day (and throw in a XS reading too).
OR just accept one is "right enough" and go with that.
I appreciate your insight into the matter and I have been doing this for over 8 years on a weekly basis. I understand the instructions for using the machine and do my best to follow the proper procedure.
I was not to know that and if you'd started with something like that I may have answered differently
pardon the out of order but:
I am not saying this is always the case for everyone, just that anyone who is home testing would benefit from occasionally verifying the accuracy of their results by using other proven testing methods.
I often recommend this here and do it myself. In my case I'm not more than 0.2 INR units out (although I was 0.5 when I first started.
Looking back on various lab tests over the last year, done at different hospital labs, there is a common trend toward the coaguchek always being significantly higher than the reported lab values when it comes to my blood.
I'm not sure what you mean by various lab tests, it could mean "various tests at the same lab" or "various labs"
I can only suggest that you can't know without taking readings within hours and documenting them so that you know it was 0.x different
There have been a few people here before who are unable to get consistent lab results but some of those have proven to vanish when they change labs.
I'm a bit confused here:
In my case, my coaguchek xs always reads significantly higher than a lab test, which has never been a problem because my inr has always been around 3.0 to 3.5 on my coaguchek, which was fine because the lab value would be anywhere from 2.3 to 2.8, though this was not known at the time.
so are you saying that when you are reading 3.0 on the XS you are seeing 2.3 at the lab? are you sure of these correlations (like you wrote them down with dates?
It has now become a problem because my new cardio wants me at a range of 2.0 to 3.0, instead of 2.5 to 3.5, which is what my old cardio had me at.
well I'm not entirely sure I see the problem especially when you don't know what a 2.0 on the XS actually correlates to from a lab (or if you do you haven't said that. Recall from the graphs above that the lower the INR the less the deviation?
I do not feel comfortable trusting my machine if it tells me my inr is 2.0 to 2.5 because this could possibly mean that my true inr is below 2.0
- conduct tests and
- I do not suggest anyone sits on 2 and
- being 2 is a signal to steer INR higher
, which we all know leads to possible complications over a longer period of time at levels below 2.0
agreed, so if you see a trend downwards from 2.5 towards 2 then steer it back up ... if you test weekly there will be no longer period of time
citing a section of "that graph"
would suggest that 6.7 events per 100 patient years is a low risk especially if you steer it up
. I have a lot more faith in hospital labs that run inr tests all day everyday, than I do in a machine that I use once a week.
up to you ... its not been my experience.
... I am hoping that my machine is broken or just old and that a new machine will correlate more closely to lab results.
I would doubt it, but it could be eliminated by finding somehwere / someone with an XS and taking your strips and code chip there and actually testing side by side.
Looking at the graph you posted, my numbers would be extreme outliers when compared to the plotted inr numbers in the graph.
not so extreme as to not appear on that graph
This is un settling to me and makes it very difficult to trust that any readings under 2.5 on the coaguchek have me in a safe inr range.
assuming you know that INR is not like measuring a peice of machined steel with a vernier caliper I suggest its not as unsettling as you feel it is.
I would suggest you follow up and also try (if you already haven't) other labs and see (if you can do so) how much variance you find between companies with a blood draw the same day (and throw in a XS reading too).
OR just accept one is "right enough" and go with that.
Hi
I was not to know that and if you'd started with something like that I may have answered differently
pardon the out of order but:
I often recommend this here and do it myself. In my case I'm not more than 0.2 INR units out (although I was 0.5 when I first started.
I'm not sure what you mean by various lab tests, it could mean "various tests at the same lab" or "various labs"
I can only suggest that you can't know without taking readings within hours and documenting them so that you know it was 0.x different
There have been a few people here before who are unable to get consistent lab results but some of those have proven to vanish when they change labs.
I'm a bit confused here:
so are you saying that when you are reading 3.0 on the XS you are seeing 2.3 at the lab? are you sure of these correlations (like you wrote them down with dates?
well I'm not entirely sure I see the problem especially when you don't know what a 2.0 on the XS actually correlates to from a lab (or if you do you haven't said that. Recall from the graphs above that the lower the INR the less the deviation?
- conduct tests and
- I do not suggest anyone sits on 2 and
- being 2 is a signal to steer INR higher
agreed, so if you see a trend downwards from 2.5 towards 2 then steer it back up ... if you test weekly there will be no longer period of time
citing a section of "that graph"
View attachment 888295
would suggest that 6.7 events per 100 patient years is a low risk especially if you steer it up
up to you ... its not been my experience.
I would doubt it, but it could be eliminated by finding somehwere / someone with an XS and taking your strips and code chip there and actually testing side by side.
not so extreme as to not appear on that graph
View attachment 888296
assuming you know that INR is not like measuring a peice of machined steel with a vernier caliper I suggest its not as unsettling as you feel it is.
I would suggest you follow up and also try (if you already haven't) other labs and see (if you can do so) how much variance you find between companies with a blood draw the same day (and throw in a XS reading too).
OR just accept one is "right enough" and go with that.
I appreciate your discussion on the matter and I will take your advice and try and find another coaguchek xs to compare to my coaguchek xs.
Thanks
Warrick
Well-known member
FWIW my lab uses coaguchek meters which I believe the calibration is checked daily with some sort of test fluid. I check my meter against theres every 12 months or so and its varied from exactly the same to 0.3 difference, so im happy with that.
I did google the test fluid and found this for NZ
https://www.nzonlinechemist.co.nz/p...MIofnUn_Hu9AIV1BwrCh15oAazEAQYASABEgL42fD_BwESo maybe its something to look into I think it does specifie for a specific model of meter but if they are all using the same strips which is where the reagent is then I cant see why it couldnt work on any coaguchek.
I did google the test fluid and found this for NZ
https://www.nzonlinechemist.co.nz/p...MIofnUn_Hu9AIV1BwrCh15oAazEAQYASABEgL42fD_BwESo maybe its something to look into I think it does specifie for a specific model of meter but if they are all using the same strips which is where the reagent is then I cant see why it couldnt work on any coaguchek.
My experience with this is that lab results also differ from lab to lab depending upon method used. When I was regularly lab testing post surgery, I used two different labs and then immediately tested at home to ensure that I was confident in my abilities to manage the coaguchek. As it turned out, the coaguchek was always .2 to .3 above the reading from one of the labs I used, but always bang on to the other lab.
I do know from previous threads on this that different lab procedures give differing results.
I don’t know which reading is more accurate, but this still gave me confidence with my meter as I am working within a range. My range is 2-3. I shoot for 2.5.
I do know from previous threads on this that different lab procedures give differing results.
I don’t know which reading is more accurate, but this still gave me confidence with my meter as I am working within a range. My range is 2-3. I shoot for 2.5.
About the same experience here with my wife's XS:As it turned out, the coaguchek was always .2 to .3 above the reading from one of the labs I used, but always bang on to the other lab.
"INR from lab was lower than results from the XS 24 out of 25 times, on average, .338 lower (i.e. so on average, if XS reported 3.0, the lab reported 2.7 - rounded up)."
Coag-Sense versus CoaguChek xs and labs
pellicle
Professional Dingbat, Guru and Merkintologist
a further point has emerged from another discussion I'm having.
@Cmf2p are you using alcohol to clean your finger if you are DO NOT
the manual once upon a time mentioned doing that but made it explicit:

the orange strike through is removed from modern manuals now as far as I can see. Why? well because any contamination on the skin WILL change the readings as the manual further mentions here:

myself I strongly urge that you follow the methods as I outlined them in this thread
https://www.valvereplacement.org/threads/coaugcheck-vs-coaugusence.888344/post-912845
@Cmf2p are you using alcohol to clean your finger if you are DO NOT
the manual once upon a time mentioned doing that but made it explicit:
the orange strike through is removed from modern manuals now as far as I can see. Why? well because any contamination on the skin WILL change the readings as the manual further mentions here:
myself I strongly urge that you follow the methods as I outlined them in this thread
https://www.valvereplacement.org/threads/coaugcheck-vs-coaugusence.888344/post-912845
Superman
Well-known member
I just don’t go to the lab. Problem solved. 
Warrick
Well-known member
I hear ya... and second that 
- Joined
- Dec 21, 2021
- Messages
- 101
Firstly how much experience do you have with the machine? I found that when I first started my reproduction was a bit haphazard. Remember you are being a technician here, not just changing channels with a remote control. You need to make sure that:
If you "milk" your finger would that cause the INR result to be lower or higher? I wonder if this is why I am lower than usual. I am always cold this time of year and I do keep my hands under hot water before testing but I am guilty of "milking".
- you are strictly following the directions, including (perhaps especially) the 15 second rule
- you are not milking the finger excessively (which can trigger thrombosis to have started already)
- you are not using the same lance site for subsequent readings (because this will pollute the readings)
If you "milk" your finger would that cause the INR result to be lower or higher? I wonder if this is why I am lower than usual. I am always cold this time of year and I do keep my hands under hot water before testing but I am guilty of "milking".
A few years ago, I did extensive testing with many different machines, looking for the meter that I would trust with my life.
I compared results from each meter to the results of the other meters, and also to the lab results.
Over the years, I've also run into grossly wrong lab results - bad technique, bad handling of the blood after it's drawn, and probably other issues, too.
For many years, I believed (and trusted) the Coag-Sense as the most accurate meter for my purposes.
For comparison, I added the CoaguChek to my testing protocol, just to see which seemed to be most accurate.
I also occasionally compared both to the labs.
Surprisingly (to me) was that there was a difference of up to 1.0 between Coag-Sense and CoaguChek - and for most lab tests, the CoaguChek seemed to be closest to the labs.
The last lab test had results that almost matched my Coag-Sense.
The difference between Coag-Sense and CoaguChek increased as my INR increased.
At this point, as long as the Coag-Sense shows an INR above 2.5 or so, I'm comfortable. If the CoaguChek shows an INR around 3.0, I'm comfortable.
As long as I'm confident that my INR is above 2.0 (and closer to 2.5), I'm comfortable with the result.
EVEN IF my INR is actually closer to 4.0, it's not a big deal -- clotting will take marginally longer, but it's not going to change my life or how I'm wasting it.
You can't 'calibrate' either meter - you can do quality tests against reagents to verify a strip's reading - but you can't calibrate it.
Both types of meters have built-in quality controls, and both have codes that apply only to a strip (or batch of strips). These are adjustments, based on reagent values, that make the results accurate. On the CoaguChek, it's in a code chip that comes with the strips. The Coag-Sense has the value imprinted on the strip.
These meters are made for labs, as well as for home testers. Potentially, they can run thousands of tests without error - any consistent pattern of errors can be particularly damaging to the manufacturer of the meters - both in human life and in legal/reputation damage. FDA may also force the removal of the meters from the market (this happened a few years ago to the dreadful Hemosense meter). Meter manufacturers are DAMNED careful to assure that their meters are ALWAYS accurate (or within a certain range or accuracy).
I wouldn't worry about using an old meter. Mine is old. I just bought another, and the results match (almost) on both meters.
Personally, I would aim for an INR of 3.0 or higher on my CoaguChek, and feel comfortable that I have an adequate, safe, INR.
As for milking the finger - this DOES make a difference. Diluting the clotting factors with plasma might change the results.
I compared results from each meter to the results of the other meters, and also to the lab results.
Over the years, I've also run into grossly wrong lab results - bad technique, bad handling of the blood after it's drawn, and probably other issues, too.
For many years, I believed (and trusted) the Coag-Sense as the most accurate meter for my purposes.
For comparison, I added the CoaguChek to my testing protocol, just to see which seemed to be most accurate.
I also occasionally compared both to the labs.
Surprisingly (to me) was that there was a difference of up to 1.0 between Coag-Sense and CoaguChek - and for most lab tests, the CoaguChek seemed to be closest to the labs.
The last lab test had results that almost matched my Coag-Sense.
The difference between Coag-Sense and CoaguChek increased as my INR increased.
At this point, as long as the Coag-Sense shows an INR above 2.5 or so, I'm comfortable. If the CoaguChek shows an INR around 3.0, I'm comfortable.
As long as I'm confident that my INR is above 2.0 (and closer to 2.5), I'm comfortable with the result.
EVEN IF my INR is actually closer to 4.0, it's not a big deal -- clotting will take marginally longer, but it's not going to change my life or how I'm wasting it.
You can't 'calibrate' either meter - you can do quality tests against reagents to verify a strip's reading - but you can't calibrate it.
Both types of meters have built-in quality controls, and both have codes that apply only to a strip (or batch of strips). These are adjustments, based on reagent values, that make the results accurate. On the CoaguChek, it's in a code chip that comes with the strips. The Coag-Sense has the value imprinted on the strip.
These meters are made for labs, as well as for home testers. Potentially, they can run thousands of tests without error - any consistent pattern of errors can be particularly damaging to the manufacturer of the meters - both in human life and in legal/reputation damage. FDA may also force the removal of the meters from the market (this happened a few years ago to the dreadful Hemosense meter). Meter manufacturers are DAMNED careful to assure that their meters are ALWAYS accurate (or within a certain range or accuracy).
I wouldn't worry about using an old meter. Mine is old. I just bought another, and the results match (almost) on both meters.
Personally, I would aim for an INR of 3.0 or higher on my CoaguChek, and feel comfortable that I have an adequate, safe, INR.
As for milking the finger - this DOES make a difference. Diluting the clotting factors with plasma might change the results.
Last edited:
pellicle
Professional Dingbat, Guru and Merkintologist
ok, I still say try my above method, not bit of it, all of it.I wonder if this is why I am lower than usual.
Next I say strictly adhere to the 15 second rule, clotting cascade has begun from the instant of lance penetration and determining clotting time is a matter of timing.
Have you noticed that if your INR is (say) 3.5 that the machine takes longer to declare this than (say) 2.5? This is because it is timing how long coagulation takes. Recall how this works;
- determine prothrombin time
- apply the ISI
- apply the formula to make INR
Be strict in your approach and you will get consistent results from your device.
I recommend you understand a bit of what is happening here, so from this:
https://www.ncbi.nlm.nih.gov/books/NBK482253/
The coagulation pathway is a cascade of events that leads to hemostasis. The intricate pathway allows for rapid healing and prevention of spontaneous bleeding. Two paths, intrinsic and extrinsic, originate separately but converge at a specific point, leading to fibrin activation. The purpose is to ultimately stabilize the platelet plug with a fibrin mesh.
key word = rapid
We are dealing with the Extrinsic pathway (something from outside)
The extrinsic pathway is the shorter pathway of secondary hemostasis. Once the damage to the vessel is done, the endothelial cells release tissue factor which goes on to activate factor VII to factor VIIa. Factor VIIa goes on to activate factor X into factor Xa. This is the point where both extrinsic and intrinsic pathways become one. The extrinsic pathway is clinically measured as the prothrombin time (PT).
so the instant that the lance penetrates the endothelial cells (capilary wall lining cells) begin to release tissue factor. Again, from that time.
This is why you MUST follow the 15 second rule. If you do not follow it then the machine can't know that, the machine can only know from the moment the blood was applied. Thus if you took 30 seconds to do this properly then the machine will think it took 15 seconds less time to clot than reality and will give you a LOW INR.
I say again, follow exactly each and every step I gave above, both in points and in the video. If you still are getting errant readings we can work through that. But doing it right isn't hard and is important.
Merry Christmas and a Happy New Year
Best Wishes
Last edited:
- Joined
- Dec 21, 2021
- Messages
- 101
ok, I still say try my above method, not bit of it, all of it.
Next I say strictly adhere to the 15 second rule, clotting cascade has begun from the instant of lance penetration and determining clotting time is a matter of timing.
Have you noticed that if your INR is (say) 3.5 that the machine takes longer to declare this than (say) 2.5? This is because it is timing how long coagulation takes. Recall how this works;
its not a magic box it is an instrument and you are the clinician. Its not complex to operate (and clinicians aren't doctors or even rocket scientists, but they ARE trained to be regular, reliably repetitive and pay attention to the rules).
- determine prothrombin time
- apply the ISI
- apply the formula to make INR
Be strict in your approach and you will get consistent results from your device.
I recommend you understand a bit of what is happening here, so from this:
https://www.ncbi.nlm.nih.gov/books/NBK482253/
The coagulation pathway is a cascade of events that leads to hemostasis. The intricate pathway allows for rapid healing and prevention of spontaneous bleeding. Two paths, intrinsic and extrinsic, originate separately but converge at a specific point, leading to fibrin activation. The purpose is to ultimately stabilize the platelet plug with a fibrin mesh.
key word = rapid
We are dealing with the Extrinsic pathway (something from outside)
The extrinsic pathway is the shorter pathway of secondary hemostasis. Once the damage to the vessel is done, the endothelial cells release tissue factor which goes on to activate factor VII to factor VIIa. Factor VIIa goes on to activate factor X into factor Xa. This is the point where both extrinsic and intrinsic pathways become one. The extrinsic pathway is clinically measured as the prothrombin time (PT).
so the instant that the lance penetrates the endothelial cells (capilary wall lining cells) begin to release tissue factor. Again, from that time.
This is why you MUST follow the 15 second rule. If you do not follow it then the machine can't know that, the machine can only know from the moment the blood was applied. Thus if you took 30 seconds to do this properly then the machine will think it took 15 seconds less time to clot than reality and will give you a LOW INR.
I say again, follow exactly each and every step I gave above, both in points and in the video. If you still are getting errant readings we can work through that. But doing it right isn't hard and is important.
Merry Christmas and a Happy New Year
Best Wishes
Thanks so much for all the information. I think part of my problem is definitely with my technique. I retested today and my INR was .2 higher putting me at least in range although still at the lower end. I used a rubber band as you suggest but must not have had it tight enough because I still didn't produce a good drop quickly. I have the Coagsense machine so I collect with a tube and then have to put it in the hole in the strip which takes a little time. Next week I have an appointment to also test with my lab. I will work hard to master this!!
Merry Christmas and Happy New Year to you as well.
pellicle
Professional Dingbat, Guru and Merkintologist
Hi
ok, so what is your INR and are you comparing it with a lab? Because if you're not comparing it with a lab, just trust the CoaguchekI retested today and my INR was .2 higher putting me at least in range although still at the lower end
- Joined
- Dec 21, 2021
- Messages
- 101
My goal range is 1.5 to 2. I was 1.3 on Wednesday but at a 1.5 on Thursday when I retested. I have not compared to a lab draw since I got my machine so want to do that next week. I really think it is my technique. I have only been using the machine for 5 weeks. I am going to try everything you suggest next week when I test including the hot shower.Hi
ok, so what is your INR and are you comparing it with a lab? Because if you're not comparing it with a lab, just trust the Coaguchek
Thanks for your help.
pellicle
Professional Dingbat, Guru and Merkintologist
Well I don't know who concocted that because the company On-x lists 1.6 as the minimum.My goal range is 1.5 to
There is a lot to that decision and one thing is not to go below 1.6 the other is co administration of aspirin. I suggest you read this post about a members problems with that protocol
https://www.valvereplacement.org/threads/failure-of-onx-valve-and-problems-with-lowering-inr.878615/
There isn't a follow up study that confirms it either, so the knowledge we have suggests it's no different (shock) to every other nearly identical bileaflet pyrolytic carbon valve.
We have a saying here ; it's easier for the body to replace blood cells than brain cells.
Best Wishes
Pellicle is right - if I had an On-X, I would STILL have a target of around 3.0. Even at 4.0, if your INR ever gets this high, living with it is no big deal. You may wind up with more bruises if you bang yourself than you might with a lower INR, but, really, it's not a big deal.
Now - regarding CoaguChek and Coag-Sense -- I find that you need a bigger drop of blood to fill the transfer tube for the Coag-Sense than you will if you just put your finger with the blood drop on the side of a CoaguChek strip and HOLD it there until the strip draws in all the blood. With a little practice, the CoaguChek may be easier than the Coag-Sense.
To get a good drop, I often hold my hand under warm/hot water for a few seconds. I sometimes swing my arm around - like a windmill - it brings the blood to the hand. I also try to not use the same finger all the time - I find that more 'virgin' areas in other fingers are less scarred and more easily yield usable drops.
I also do a thing, similar to Pellicle's rubber band or dental floss: when I'm waiting for the meter to be ready to test, I compress my finger, below the knuckle, and it usually pools enough blood in the front of the finger to give me a good drop for testing.
It's easier to stay within the fifteen second limit when I use the CoaguChek than it is with the Coag-Sense, because it takes a few seconds for the Coag-Sense transfer tube to fill with blood, and then another second or two (depending on how good your aim is) to transfer the blood onto the strip.
Now - regarding CoaguChek and Coag-Sense -- I find that you need a bigger drop of blood to fill the transfer tube for the Coag-Sense than you will if you just put your finger with the blood drop on the side of a CoaguChek strip and HOLD it there until the strip draws in all the blood. With a little practice, the CoaguChek may be easier than the Coag-Sense.
To get a good drop, I often hold my hand under warm/hot water for a few seconds. I sometimes swing my arm around - like a windmill - it brings the blood to the hand. I also try to not use the same finger all the time - I find that more 'virgin' areas in other fingers are less scarred and more easily yield usable drops.
I also do a thing, similar to Pellicle's rubber band or dental floss: when I'm waiting for the meter to be ready to test, I compress my finger, below the knuckle, and it usually pools enough blood in the front of the finger to give me a good drop for testing.
It's easier to stay within the fifteen second limit when I use the CoaguChek than it is with the Coag-Sense, because it takes a few seconds for the Coag-Sense transfer tube to fill with blood, and then another second or two (depending on how good your aim is) to transfer the blood onto the strip.
- Joined
- Dec 21, 2021
- Messages
- 101
Well I don't know who concocted that because the company On-x lists 1.6 as the minimum.
There is a lot to that decision and one thing is not to go below 1.6 the other is co administration of aspirin. I suggest you read this post about a members problems with that protocol
https://www.valvereplacement.org/threads/failure-of-onx-valve-and-problems-with-lowering-inr.878615/
There isn't a follow up study that confirms it either, so the knowledge we have suggests it's no different (shock) to every other nearly identical bileaflet pyrolytic carbon valve.
We have a saying here ; it's easier for the body to replace blood cells than brain cells.
Best Wishes
Again, I appreciate all your input. I actually received information in the mail from On-X that said the target INR range is 1.5 - 2.0. That is what is currently on their website too. I totally get what you are saying, and I am working on being closer to a 2.0. Lots to discuss at my next appointment with my cardiologist.