heartweave
Member
It has been awhile since I have written. Since then I have gotten a variety of second and third opinions, some of which contradict each other. Perhaps someone could shed light on this.
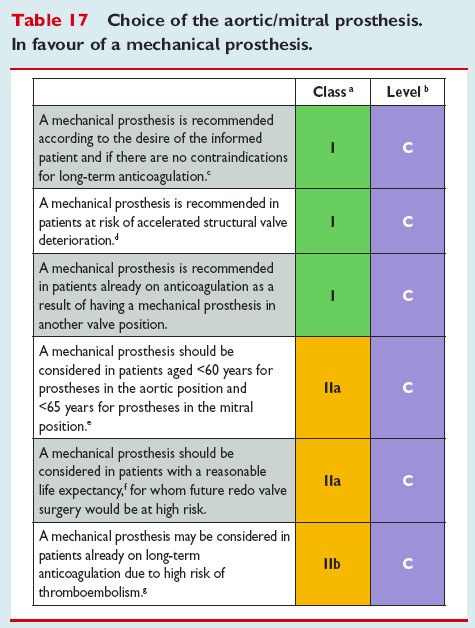
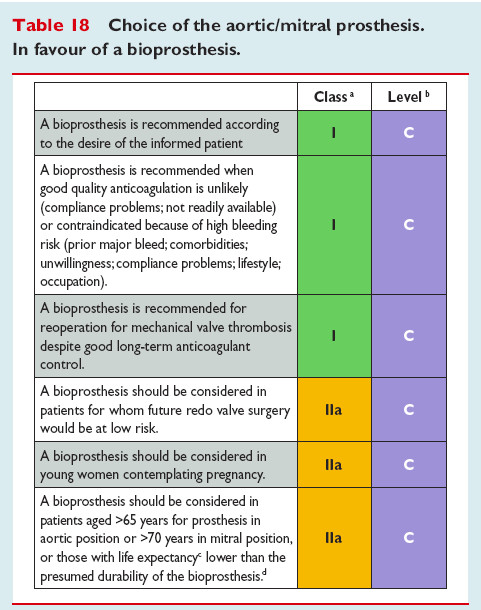
First surgeon Dr. Gaudiani….wanted to do surgery this month. My ejection is 60 but my stenosis is 0.7. He recommended biological valve. I am 58. He said don’t travel out of the country.
Second Surgeon. Dr. Craig Miller, Stanford… Redid the echo. He wondered why they hadn’t done a pulmonary function or BNP blood tests. He said the stenosis is at 0.9. He wants me on a daily beta blocker He said I do not need surgery yet. He thought probably not for a year or two. He said the fact I can exercise regularly means I am not ready for surgery. He said absolutely he would NOT consider a bio valve on someone my age. What they learned is the fail is 5-10 years. He felt I should only consider a mechanical valve and Coumadin is not that big a deal. He said I can always find someone who will say I need surgery now but….He said go have fun, enjoy life, no restrictions on traveling out of the country. Valve was leaking a bit.
Cardiologist- don’t listen to the surgeons. He is the one who sees me and decides when I need surgery. He feels the extreme fatigue is not from my heart. He said the main criteria is shortness of breath. He didn’t think I should be on a beta blocker even though I am having palpitations. He told me to look at the top hat mechanical valve that may not need Coumadin. He also said the fact that I had left sided radiation for breast cancer, it will be a mess if they have to do surgery more than once.
My primary physician told me not to consider Coumadin as it is a death sentence and it will shorten your life.
Meanwhile….I am very tired. I push myself to dance for 45 minutes to an hour but I am exhausted after. I am finding I need to take naps during the day and start falling asleep by 8pm.
I have not even done any research on the mechanical valves. I am so confused. Should I consider talking to another cardiologist. Should I just wait and keep on going back to my cardiologist. I guess I need to consider a mechanical valve .
Leah
58 year old ( on Monday), EF 60-65%, Stenosis 0.7 ot 0.9
First surgeon Dr. Gaudiani….wanted to do surgery this month. My ejection is 60 but my stenosis is 0.7. He recommended biological valve. I am 58. He said don’t travel out of the country.
Second Surgeon. Dr. Craig Miller, Stanford… Redid the echo. He wondered why they hadn’t done a pulmonary function or BNP blood tests. He said the stenosis is at 0.9. He wants me on a daily beta blocker He said I do not need surgery yet. He thought probably not for a year or two. He said the fact I can exercise regularly means I am not ready for surgery. He said absolutely he would NOT consider a bio valve on someone my age. What they learned is the fail is 5-10 years. He felt I should only consider a mechanical valve and Coumadin is not that big a deal. He said I can always find someone who will say I need surgery now but….He said go have fun, enjoy life, no restrictions on traveling out of the country. Valve was leaking a bit.
Cardiologist- don’t listen to the surgeons. He is the one who sees me and decides when I need surgery. He feels the extreme fatigue is not from my heart. He said the main criteria is shortness of breath. He didn’t think I should be on a beta blocker even though I am having palpitations. He told me to look at the top hat mechanical valve that may not need Coumadin. He also said the fact that I had left sided radiation for breast cancer, it will be a mess if they have to do surgery more than once.
My primary physician told me not to consider Coumadin as it is a death sentence and it will shorten your life.
Meanwhile….I am very tired. I push myself to dance for 45 minutes to an hour but I am exhausted after. I am finding I need to take naps during the day and start falling asleep by 8pm.
I have not even done any research on the mechanical valves. I am so confused. Should I consider talking to another cardiologist. Should I just wait and keep on going back to my cardiologist. I guess I need to consider a mechanical valve .
Leah
58 year old ( on Monday), EF 60-65%, Stenosis 0.7 ot 0.9
")